
Abstract
Trastuzumab reduces the risk of relapse in women with HER2-positive non-metastatic breast cancer, but little information exists on the timing of trastuzumab initiation. The study investigated the impact of delaying the initiation of adjuvant trastuzumab therapy for >6 months after the breast cancer diagnosis on time to relapse, overall survival (OS), and relapse-free survival (RFS) among patients with non-metastatic breast cancer. Adult women with non-metastatic breast cancer who initiated trastuzumab adjuvant therapy without receiving any neoadjuvant therapy were selected from the US Department of Defense health claims database from 01/2003 to 12/2012. Two study cohorts were defined based on the time from breast cancer diagnosis to trastuzumab initiation: >6 months and ≤6 months. The impact of delaying trastuzumab initiation on time to relapse, OS, and RFS was estimated using Cox regression models adjusted for potential confounders. Of 2749 women in the study sample, 79.9 % initiated adjuvant trastuzumab within ≤6 months of diagnosis and 20.1 % initiated adjuvant trastuzumab >6 months after diagnosis. After adjusting for confounders, patients who initiated trastuzumab >6 months after the breast cancer diagnosis had a higher risk of relapse, death, or relapse/death than those who initiated trastuzumab within ≤6 months of diagnosis (hazard ratios [95 % CIs]: 1.51 [1.22–1.87], 1.54 [1.12–2.12], and 1.43 [1.16–1.75]; respectively). The results of this population-based study suggest that delays of >6 months in the initiation of trastuzumab among HER2-positive non-metastatic breast cancer patients are associated with a higher risk of relapse and shorter OS and RFS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the most common malignancy in women and the leading cause of cancer death in women aged 20–59 years [1]. It accounts for 29 % of new cancers in American women annually, with >200,000 new cases per year [1]. Today, breast cancer is detected in most patients in the early stages of disease progression [2–5]. The most common treatment for such patients includes tumor removal surgery and adjuvant systemic therapy intended to kill any cancer cells left behind [6, 7].
In November 2006, the FDA approved trastuzumab as adjuvant therapy for HER2-positive breast cancer [8, 9], a subtype of breast cancer that carries an increased risk of recurrence and overall poor prognosis. The introduction of trastuzumab has dramatically improved the management of HER2-positive breast cancer. The efficacy and effectiveness of adjuvant trastuzumab in this population has been confirmed in multiple clinical trials [10–17] and observational studies [18–26]. Yet, little is known about the timing of trastuzumab initiation and its impact on patient outcomes.
Several retrospective studies have evaluated the role of delayed adjuvant therapy in patients with breast cancer of all types, reporting mixed results. When treatment delay was defined as ≥12 weeks following surgery, a positive relationship was found between delay and the risk of death [27–29]. When shorter time intervals were used, most studies found null associations [30–32], although one study found that starting adjuvant therapy within 21 days from the surgery date had a beneficial effect [33]. Additionally, a recent meta-analysis concluded that the risk of death increased by 15 % for each 4-week delay in adjuvant breast cancer therapy initiation [34]. However, few of these studies have accounted for the time from diagnosis to surgery, an integral component of the delay in the initiation of adjuvant therapy. Furthermore, the studies that did account for the time from diagnosis to surgery excluded patients with delays in surgery [27, 28], limiting the generalizability of the results.
Literature is heterogeneous, not only in definitions of delay in adjuvant therapy, but also in terms of patient, disease, and treatment characteristics. Since HER2 amplification is associated with more aggressive tumor biology, the impact of treatment delay may be different for these patients. To our best knowledge, only one study [35] has investigated the optimal time to adjuvant therapy initiation among patients with HER2-positive breast cancer receiving trastuzumab, concluding that patients who initiated adjuvant therapy >60 days after breast cancer surgery had a threefold increase in the risk of death relative to patients initiating therapy <30 days after surgery (hazard ratio 3.09, p = 0.002). However, further studies with contemporary samples of patients are needed in order to confirm these findings.
This study aimed to investigate the impact of delaying the initiation of adjuvant trastuzumab therapy after the diagnosis of cancer on the risk of relapse, overall survival (OS), and relapse-free survival (RFS) in a contemporary sample of patients with HER2-positive non-metastatic breast cancer who were neoadjuvant naïve prior to surgery.
Methods
Data sources
The US Department of Defense (DOD) Military Health System (MHS) comprised several databases that include comprehensive information on the health care and services provided to >9.5 million active beneficiaries of TRICARE insurance such as DOD service members, retirees, and their dependents [36]. The study used the following MHS data sources: (a) the Defense Enrollment Eligibility Reporting System (DEERS) database that includes demographic characteristics of the TRICARE enrollees; (b) the MHS Data Repository (MDR) claims databases that include both claims-per-service data for inpatient and outpatient health services delivered in military or civilian facilities through the TRICARE healthcare plan, and medication prescriptions for all TRICARE beneficiaries; and (c) the Automated Central Tumor Registry (ACTUR) that includes records on the cancer characteristics and cancer recurrences of all cancer cases followed by the DOD military facilities. Data used in this study covered the period from January 1, 2003 to December 31, 2012. All DOD databases were linked through identity-masked unique patient identifiers. Research data were derived from an approved Naval Medical Center, Portsmouth, VA Institutional Review Board protocol and comply with the requirements of the Health Insurance Portability and Accountability Act.
Study design and outcomes
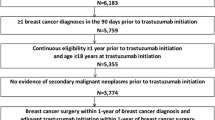
The study included patients with non-metastatic breast cancer who did not receive neoadjuvant therapy (chemotherapy, targeted, or hormonal) and were initiated on adjuvant trastuzumab alone or in combination with other adjuvant chemotherapy or targeted agents within 1 year of breast cancer surgery (N = 2749, Fig. 1).

Sample selection flowchart. aInternational statistical classification of diseases, 9th revision, clinical modification [ICD-9-CM] code 174.x; bFrom January 1, 2003 to December 31, 2012; cTwo consecutive diagnoses of secondary neoplasms (ICD-9-CM 196.x-199.x, excluding codes that may be used to indicate locally advanced breast cancer: 196.0, 196.1, 196.3, and 198.2), within 60 days of each other; dChemotherapy, targeted or hormonal therapy
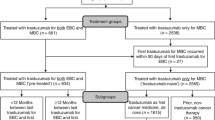
The study used a retrospective cohort design (Fig. 2). The date of the adjuvant trastuzumab initiation, which corresponds to the first trastuzumab infusion received by the patient after the diagnosis, was defined as the index date. Two study cohorts were defined based on the time from the breast cancer diagnosis to the index date: (a) the >6 months (“delay”) cohort (n = 552) and (b) the ≤6 months (“no delay”) cohort (n = 2197). The delay in trastuzumab therapy was defined from the breast cancer diagnosis rather than the breast cancer surgery because delays in surgery are an inherent part of the delays in the initiation of trastuzumab therapy, and the aim of the study was to investigate the impact of delays in trastuzumab therapy initiation, regardless of the reasons for the delays. The 6-month cut-off used to define delay in trastuzumab therapy initiation was selected based on clinical expertise to allow for sequential therapy with surgery and trastuzumab.

Study design. aTrastuzumab was first approved in 1998 for the treatment of breast cancer in the metastatic setting, and then approved in 2006 in the adjuvant setting; the study included 494 patients without evidence of metastatic disease who received trastuzumab between 2003 and 2006. bAdjuvant regimen type was identified based on the chemotherapy and/or targeted therapies received in the period between the breast cancer surgery and 28 days after the initiation of trastuzumab. OS overall survival, RFS relapse-free survival
The three outcomes of this study were time to relapse, OS, and RFS. Relapses were identified in the DOD claims data using an algorithm based on diagnoses of secondary malignant neoplasms (using International statistical classification of diseases, 9th revision, clinical modification [ICD-9-CM] diagnosis codes), treatment gaps, and treatment initiations, which was developed by the study authors by adapting three previously published algorithms [37–39] to the specifics of adjuvant trastuzumab treatment in non-metastatic breast cancer [40]. Deaths were identified from the demographic records in the DEERS database. All three outcomes were measured and compared between the study cohorts from the index date to the end of data availability (December 31, 2012) or the end of continuous healthcare coverage. Patients’ observation periods were censored if they reached the end of the database follow-up or of continuous healthcare coverage without having the event of interest (relapse and/or death). For the relapse-only outcome, patients were also censored at the time of death.
Statistical analyses
In unadjusted analyses, the relapse, death, and relapse/death outcomes were compared between study cohorts using Chi-square tests, while Kaplan–Meier plots were used to describe the time to relapse, OS, and RFS (3- and 5-year rates were reported). Outcomes were also compared between study cohorts using unadjusted Cox regression models which yielded unadjusted hazard ratios (HRs) and 95 % confidence intervals (CIs).
In adjusted analyses, outcomes were compared between study cohorts using multivariate Cox regression models adjusted for the patient’s age at diagnosis, Charlson comorbidity index (CCI) [41], the type of breast cancer surgery (breast conserving vs. breast removing), the use of neoadjuvant and adjuvant radiation therapy prior to the initiation of trastuzumab, the use of adjuvant hormonal therapy prior to the initiation of trastuzumab, and the type of adjuvant therapy regimen (ACTHFootnote 1-like, TCHFootnote 2-like, trastuzumab monotherapy, trastuzumab + taxanes, and other trastuzumab-based regimens). Adjusted HRs and 95 % CIs were reported. The proportionality of hazards (PH) assumption was tested by the interaction between the study cohorts and time and by investigating the crossing of curves in the Kaplan–Meier plots. Violations of the PH assumption for all three outcomes indicated that the HR for “delay” versus “no delay” cohort has changed approximately 1 year after the index date. Therefore, the Cox regression models were also estimated separately for the period from index date to 1 year post index date (Period 1) and the period from 1 year post index date to the end of follow-up (Period 2).
Two sensitivity analyses were conducted: one where the “delay” and “no delay” cohorts were defined by the time from diagnosis to adjuvant therapy initiation (instead of trastuzumab initiation) using the same cut-off as in the main analysis (≤6 months and >6 months) and the other one where cohorts were defined by the time from diagnosis to adjuvant therapy initiation using a 4-month cut-off (≤4 months and >4 months).
Results
Of 2749 women who met the study selection criteria, the median time from breast cancer diagnosis to trastuzumab initiation was 3.7 months; 552 (20.1 %) were in the >6 months (“delay”) cohort, and 2197 (79.9 %) were in the ≤6 months (“no delay”) cohort (Fig. 1).
Prior to trastuzumab treatment, the study cohorts did not differ in the type of surgery received (Table 1). However, the treatments received prior to the index date differed between the study cohorts: adjuvant hormonal therapy prior to trastuzumab was used by 22.1 % of the patients in the “delay” versus 4.8 % patients in the “no delay” cohort (p < 0.001), and radiation therapy was used by 74.1 % of the patients in the “delay” versus 52.3 % patients in the “no delay” cohort (p < 0.001, used in adjuvant setting by 97.2 % of the users). The trastuzumab-based adjuvant therapy regimens also varied between the cohorts, with ACTH-like regimens being the most common regimens used in the “delay” cohort (41.3 %) and TCH-like regimens, the most common regimens in the “no delay” cohort (37.2 %, Table 1).
Impact of delays in trastuzumab therapy on the risk of relapse, OS, and RFS
Over a median follow-up of 3.4 years (inter-quartile range 1.7–5.5 years), 467 relapses and 202 deaths were recorded among the 2749 patients in the study sample, and the frequency of these events was higher in the “delay” cohort versus the “no delay” cohort: 24.3 versus 15.2 % patients experienced a relapse, 11.6 versus 6.3 % patients died, and 26.8 versus 17.6 % patients either had a relapse or died (p < 0.001 for all outcomes, Table 2).
The RFS Kaplan–Meier curves presented in Fig. 3 suggest the RFS rates were similar between the study cohorts in the first year after trastuzumab initiation, but the RFS of patients in the “delay” cohort became lower than that of the patients in the “no delay” cohort afterward (log-rank p = 0.007 across the full follow-up). At 3 years after trastuzumab initiation, the unadjusted RFS rates and 95 % CIs were 75.0 % (70.9–78.6) in the “delay” cohort versus 81.2 % (79.2–82.9) in the “no delay” cohort. At 5 years, the corresponding RFS rates and 95 % CIs were 69.8 % (65.4–73.8) and 76.4 % (74.0–78.5, Fig. 3).

Comparison of unadjusted RFS between study cohorts. RFS relapse-free survival
In the overall unadjusted analyses, the risks of relapse, death, or relapse/death were significantly higher for patients in the “delay” versus “no delay” cohort (unadjusted HRs, 95 % CIs: 1.37, 1.12–1.67; 1.36, 1.01–1.83; and 1.30, 1.07–1.57; respectively, results not shown). After adjusting for potential confounding factors, the risks remained significantly higher for the “delay” versus the “no delay” cohort (adjusted HRs, 95 % CIs: 1.51, 1.22–1.87; 1.54, 1.12–2.12; and 1.43, 1.16–1.75; respectively, Table 2). The results of the full Cox regression models from the overall adjusted main analyses are presented in eTable 1.
Adjusted analyses were also replicated in Periods 1 and 2 to account for violations of the PH assumption. In Period 1, there were no statistically significant differences between the study cohorts for all three outcomes (Table 2). However, in Period 2, the adjusted analyses found increased risks of relapse, death, or relapse/death for patients in the “delay” versus “no delay” cohort (adjusted HR 1.82, 95 % CI 1.40–2.36; adjusted HR 1.67, 95 % CI 1.18–2.35; and adjusted HR 1.68, 95 % CI 1.31–2.15; respectively, Table 2).
The effect of delay was also stronger in sensitivity analyses where treatment delay was defined as >6 months from diagnosis to adjuvant therapy initiation. However, in sensitivity analyses where delay in initiation of adjuvant trastuzumab was defined as >4 months from diagnosis to adjuvant therapy initiation, the effect was weaker, regardless of the model used (Table 2).
Discussion
In this community sample of TRICARE beneficiaries, one in five women diagnosed with HER2-positive non-metastatic breast cancer initiated adjuvant trastuzumab >6 months after breast cancer diagnosis. Patients who experienced a delay in therapy initiation of >6 months after diagnosis had a higher risk of relapse, death, or relapse/death than patients who initiated trastuzumab ≤6 months after diagnosis; this higher risk became apparent 1 year after initiation of the trastuzumab treatment.
Since most previous studies did not provide information on the HER2 status of patients and used different definitions of delays in treatment, direct comparison of results is difficult. The only study investigating the impact of therapy delay among trastuzumab-treated patients with HER2-positive breast cancer found a higher risk of death among patients initiating adjuvant therapy >60 days after breast surgery compared with those initiating therapy within 30 days of surgery [35]. These results support the current study’s finding of an increased mortality risk associated with delays in the initiation of adjuvant therapy after breast cancer diagnosis. A few other studies that stratified the analyses by hormone receptor (ER) status, another factor associated with worse prognosis [28, 33], had mixed results. Lohrisch et al. [28] found that delays of >12–24 weeks (vs. ≤12 weeks) in chemotherapy initiation after surgery were associated with significantly worse OS only in ER-positive patients. However, Colleoni et al. [33] found that chemotherapy initiation in node-positive patients within 21–86 days (vs. <21 days) of surgery had a detrimental effect on OS in ER-negative but not in ER-positive patients. Nevertheless, the current study adds to the results of prior studies [33, 35], suggesting that patients with more aggressive breast cancer subtypes may benefit most from early therapy. However, further analyses stratifying patients by prognostic factors at diagnosis would be necessary to confirm this hypothesis.
Previous studies also used different cut-offs to define delays in treatment, such as >21 days [30], 21–86 days [33], 36–89 days [31], >9 weeks [32], 12–24 weeks [28], and >3 months [27, 29] after surgery. In general, studies with short cut-offs did not find an association between delays in adjuvant therapy and OS and/or RFS [30–32], while treatment delay was associated with a significant increase in the risk of death and/or relapse in studies with longer cut-offs [27–29]. Nevertheless, even short delays post-surgery (of 21–86 days among ER-negative patients [33] or of >60 days among HER2-positive patients [35]) were associated with an increase in the risk of death/relapse. Overall, these results suggest that the longer the delay in the initiation of adjuvant therapy and the more aggressive the tumor type, the stronger the impact of the delay in treatment on relapse, OS, and RFS outcomes. In the first sensitivity analysis, where delay was defined based on the time to adjuvant therapy initiation rather than time to trastuzumab initiation, the effect was generally stronger, suggesting that a delay in adjuvant therapy initiation of >6 months had a substantial impact on the risk of relapse and death. Conversely, in the sensitivity analysis where cohorts were defined based on a delay of 4 months between diagnosis and adjuvant therapy initiation, the overall impact was weaker, and the impact on the risk of death lost statistical significance.
Importantly, most studies to date defined adjuvant therapy delay using the date of surgery, whereas the current study’s definition uses the breast cancer diagnosis date. Study designs that define therapy delay as starting with the date of surgery ignore the inevitable association between delays in surgery and delays in the initiation of adjuvant therapy among patients who do not receive neoadjuvant therapy (i.e., patients in whom delays in surgery are not justified by the need to downsize a large tumor). If delays in surgery are correlated with delays in adjuvant therapy or reduce the benefits of adjuvant therapy, ignoring the delay in surgery could bias estimates of mortality risks. To address this limitation, two prior studies [27, 28] excluded patients with long intervals between the diagnosis and the surgery (>6 months [27] and >17 weeks [28]). This approach, however, limited the results’ generalizability.
In the current study, the time to adjuvant trastuzumab therapy was defined as a combination of three intervals: the time between (1) diagnosis and surgery, (2) surgery and adjuvant therapy initiation, and (3) adjuvant therapy initiation and the first trastuzumab treatment (applicable to ACTH and other chemotherapy regimens with delayed trastuzumab initiation). The study did not attempt to identify the individual effect of each interval on patients’ outcomes. While this approach has limitations, the result is more generalizable for clinical practice: regardless of the timing of the surgery, initiation of adjuvant therapy >6 months following the breast cancer diagnosis might worsen OS and RFS in patients with HER2-positive tumors. Exploratory analyses among the 552 patients in the “delay” cohort suggested that patterns of delay may be treatment specific: depending on the treatment regimen, the interval accounting for most of the delay was either the time from diagnosis to surgery (i.e., TCH-like regimens, median 4.8 months) or the time from surgery to adjuvant therapy initiation (i.e., trastuzumab monotherapy, median 7.6 months; trastuzumab + taxanes, median 4.7 months) or the time from adjuvant therapy initiation to first trastuzumab (i.e., ACTH-like regimens, median 4.6 months). However, further studies are needed to investigate factors driving these delays. Clinical factors may include post-operation complications, plastic surgery procedures, or adverse effects of therapies initiated prior to trastuzumab; non-clinical factors, which are more amenable to interventions, may include wait times for imaging procedures and appointments with reconstructive plastic surgeons or fertility specialists, personal preferences for seeking second opinions, or financial and geographical constraints.
In this study sample, 11.2 % of the patients received adjuvant trastuzumab monotherapy as their first treatment after breast cancer surgery. A minority of patients who refuse chemotherapy may be directed toward trastuzumab monotherapy, while others may have comorbidities that limit their potential use of chemotherapies. However, it is unlikely that these factors alone explain the use of trastuzumab monotherapy in the study sample. Further studies are needed to understand the selection of trastuzumab monotherapy treatment in certain patients. Another finding was that 51.9 % of the patients in the study sample had mastectomies, that is more than the <50 % benchmark proposed by the America College of Surgeons/National Accreditation Program for Breast Centers [44]. However, >50 % of the patients in the study had stage II or III disease, a slightly higher percentage than the general population initially diagnosed with breast cancer [45]. In addition, these patients did not receive neoadjuvant chemotherapy to reduce the size of the primary tumor, which may have made successful breast conservation surgery more difficult.
This study was subject to the general limitations of claims data, such as occasional coding inaccuracies. These likely affect both study cohorts to a similar extent and may result in a dilution of the observed effect for the delay of trastuzumab treatment. Additionally, since this is a claims-based observational study, some potential confounders may not have been measured and adjusted for in the analyses. Other study limitations include the identification of relapses through a claims-based algorithm that relies on diagnoses of secondary neoplasms, treatment interruption, and treatment re-initiations. While this algorithm was shown to have 90 % sensitivity and 90 % specificity when validated against the recurrence records from the ACTUR [40], some misclassification of relapse events could have occurred. Second, adjuvant therapy regimens were identified from claims based on the chemotherapy and targeted agents used from breast cancer surgery up to 28 days after trastuzumab initiation, and therefore, some misclassification of the adjuvant therapy regimens is possible. Third, patients treated with neoadjuvant therapy were excluded because delays in surgery/initiation of adjuvant trastuzumab therapy may be justified when treating locally advanced disease or large tumors. However, only <15 % of the sample was excluded based on this criterion. Finally, a 6-month cut-off was used to define “delays” in trastuzumab therapy initiation. The optimal time of treatment initiation may vary based on patient characteristics, some of which are unobservable, and a single cut-off at 6 months post diagnosis may result in some misclassification of the patients in the “delay” versus “no delay” cohorts. However, the effect of delay weakened in the sensitivity analyses with a shorter cut-off (4 months), suggesting a longer cut-off is more likely to capture the impact of treatment delays on relapse and/or death outcomes.
Conclusion
In a contemporary sample of patients with non-metastatic breast cancer covered by US Department of Defense insurance, the study found that one in five patients had delays of >6 months in the initiation of adjuvant trastuzumab therapy and that these delays were associated with higher risks of death and relapse. Together with findings from prior studies, these results suggest that delays in the initiation of adjuvant treatment may be particularly harmful in patients with more aggressive tumor types. Furthermore, the study findings also suggest that the risk was higher when the delay was defined using a longer cut-off (i.e., 6 months post diagnosis instead of 4 months post diagnosis). Further studies are warranted to explore the optimal time of treatment for specific subtypes of breast cancer and to identify the factors driving delays in adjuvant trastuzumab therapy initiation.
References
Siegel R, Naishadham D, Jemal A (2013) Cancer statistics, 2013. CA Cancer J Clin 63:11–30. doi:10.3322/caac.21166
National Cancer Institute (2014) SEER cancer statistics factsheets: breast cancer. In: Surveillance, epidemiology, and end results program. http://seer.cancer.gov/statfacts/html/breast.html. Accessed 23 Sep 2014
Walters S, Maringe C, Butler J et al (2013) Breast cancer survival and stage at diagnosis in Australia, Canada, Denmark, Norway, Sweden and the UK, 2000–2007: a population-based study. Br J Cancer 108:1195–1208. doi:10.1038/bjc.2013.6
Sant M, Allemani C, Capocaccia R et al (2003) Stage at diagnosis is a key explanation of differences in breast cancer survival across Europe. Int J Cancer 106:416–422. doi:10.1002/ijc.11226
Allemani C, Sant M, Weir HK et al (2013) Breast cancer survival in the US and Europe: a CONCORD high-resolution study. Int J Cancer 132:1170–1181. doi:10.1002/ijc.27725
National Comprehensive Cancer Network (NCCN) (2014) NCCN: clinical practice guidelines in oncology—breast cancer. National Comprehensive Cancer Network (NCCN), Fort Washington, PA
van Herk-Sukel MPP, van de Poll-Franse LV, Creemers G-J et al (2013) Major changes in chemotherapy regimens administered to breast cancer patients during 2000–2008 in the Netherlands. Breast J 19:394–401. doi:10.1111/tbj.12125
Parise CA, Bauer KR, Brown MM, Caggiano V (2009) Breast cancer subtypes as defined by the estrogen receptor (ER), progesterone receptor (PR), and the human epidermal growth factor receptor 2 (HER2) among women with invasive breast cancer in California, 1999–2004. Breast J 15:593–602. doi:10.1111/j.1524-4741.2009.00822.x
Genentech I (2014) Herceptin (trastuzumab) BLA no. 103792. U.S. Food and Drug Administration, South San Francisco, CA
Romond EH, Perez EA, Bryant J et al (2005) Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 353:1673–1684. doi:10.1056/NEJMoa052122
Gianni L, Dafni U, Gelber RD et al (2011) Treatment with trastuzumab for 1 year after adjuvant chemotherapy in patients with HER2-positive early breast cancer: a 4-year follow-up of a randomised controlled trial. Lancet Oncol 12:236–244. doi:10.1016/S1470-2045(11)70033-X
Joensuu H, Kellokumpu-Lehtinen P-L, Bono P et al (2006) Adjuvant docetaxel or vinorelbine with or without trastuzumab for breast cancer. N Engl J Med 354:809–820. doi:10.1056/NEJMoa053028
Perez EA, Romond EH, Suman VJ et al (2011) Four-year follow-up of trastuzumab plus adjuvant chemotherapy for operable human epidermal growth factor receptor 2-positive breast cancer: joint analysis of data from NCCTG N9831 and NSABP B-31. J Clin Oncol 29:3366–3373. doi:10.1200/JCO.2011.35.0868
Burstein HJ, Piccart-Gebhart MJ, Perez EA et al (2012) Choosing the best trastuzumab-based adjuvant chemotherapy regimen: should we abandon anthracyclines? J Clin Oncol 30:2179–2182. doi:10.1200/JCO.2012.42.0695
Fountzilas G, Dafni U, Papadimitriou C et al (2014) Dose-dense sequential adjuvant chemotherapy followed, as indicated, by trastuzumab for one year in patients with early breast cancer: first report at 5-year median follow-up of a Hellenic Cooperative Oncology Group randomized phase III trial. BMC Cancer 14:515. doi:10.1186/1471-2407-14-515
Slamon D, Eiermann W, Robert N et al (2011) Adjuvant trastuzumab in HER2-positive breast cancer. N Engl J Med 365:1273–1283. doi:10.1056/NEJMoa0910383
Valachis A, Mauri D, Polyzos NP et al (2011) Trastuzumab combined to neoadjuvant chemotherapy in patients with HER2-positive breast cancer: a systematic review and meta-analysis. Breast 20:485–490. doi:10.1016/j.breast.2011.06.009
Zurawska U, Baribeau DA, Giilck S et al (2013) Outcomes of her2-positive early-stage breast cancer in the trastuzumab era: a population-based study of Canadian patients. Curr Oncol 20:e539–e545. doi:10.3747/co.20.1523
Vici P, Pizzuti L, Natoli C et al (2014) Outcomes of HER2-positive early breast cancer patients in the pre-trastuzumab and trastuzumab eras: a real-world multicenter observational analysis. The RETROHER study. Breast Cancer Res Treat 147:599–607. doi:10.1007/s10549-014-3133-1
Peterson DJ, Truong PT, Sadek BT et al (2014) Locoregional recurrence and survival outcomes by type of local therapy and trastuzumab use among women with node-negative, HER2-positive breast cancer. Ann Surg Oncol. doi:10.1245/s10434-014-3767-6
Palmieri C, Shah D, Krell J et al (2011) Management and outcome of HER2-positive early breast cancer treated with or without trastuzumab in the adjuvant trastuzumab era. Clin Breast Cancer 11:93–102. doi:10.1016/j.clbc.2011.03.001
Hayashi N, Niikura N, Yamauchi H et al (2013) Adding hormonal therapy to chemotherapy and trastuzumab improves prognosis in patients with hormone receptor-positive and human epidermal growth factor receptor 2-positive primary breast cancer. Breast Cancer Res Treat 137:523–531. doi:10.1007/s10549-012-2336-6
Bonifazi M, Franchi M, Rossi M et al (2014) Long term survival of HER2-positive early breast cancer treated with trastuzumab-based adjuvant regimen: a large cohort study from clinical practice. Breast. doi:10.1016/j.breast.2014.05.022
Jensen JD, Knoop A, Laenkholm AV et al (2012) PIK3CA mutations, PTEN, and pHER2 expression and impact on outcome in HER2-positive early-stage breast cancer patients treated with adjuvant chemotherapy and trastuzumab. Ann Oncol 23:2034–2042. doi:10.1093/annonc/mdr546
Webster RM, Abraham J, Palaniappan N et al (2012) Exploring the use and impact of adjuvant trastuzumab for HER2-positive breast cancer patients in a large UK cancer network. Do the results of international clinical trials translate into a similar benefit for patients in South East Wales? Br J Cancer 106:32–38. doi:10.1038/bjc.2011.506
Inwald EC, Ortmann O, Zeman F et al (2014) Guideline concordant therapy prolongs survival in HER2-positive breast cancer patients: results from a large population-based cohort of a cancer registry. Biomed Res Int 2014:137304. doi:10.1155/2014/137304
Hershman DL, Wang X, McBride R et al (2006) Delay of adjuvant chemotherapy initiation following breast cancer surgery among elderly women. Breast Cancer Res Treat 99:313–321. doi:10.1007/s10549-006-9206-z
Lohrisch C, Paltiel C, Gelmon K et al (2006) Impact on survival of time from definitive surgery to initiation of adjuvant chemotherapy for early-stage breast cancer. J Clin Oncol 24:4888–4894. doi:10.1200/JCO.2005.01.6089
Nurgalieva ZZ, Franzini L, Morgan RO et al (2013) Impact of timing of adjuvant chemotherapy initiation and completion after surgery on racial disparities in survival among women with breast cancer. Med Oncol 30:419. doi:10.1007/s12032-012-0419-1
Shannon C, Ashley S, Smith IE (2003) Does timing of adjuvant chemotherapy for early breast cancer influence survival? J Clin Oncol 21:3792–3797. doi:10.1200/JCO.2003.01.073
Cold S, Düring M, Ewertz M et al (2005) Does timing of adjuvant chemotherapy influence the prognosis after early breast cancer? Results of the Danish Breast Cancer Cooperative Group (DBCG). Br J Cancer 93:627–632. doi:10.1038/sj.bjc.6602734
Jara Sánchez C, Ruiz A, Martín M et al (2007) Influence of timing of initiation of adjuvant chemotherapy over survival in breast cancer: a negative outcome study by the Spanish Breast Cancer Research Group (GEICAM). Breast Cancer Res Treat 101:215–223. doi:10.1007/s10549-006-9282-0
Colleoni M, Bonetti M, Coates AS et al (2000) Early start of adjuvant chemotherapy may improve treatment outcome for premenopausal breast cancer patients with tumors not expressing estrogen receptors. The International Breast Cancer Study Group. J Clin Oncol 18:584–590
Yu K-D, Huang S, Zhang J-X et al (2013) Association between delayed initiation of adjuvant CMF or anthracycline-based chemotherapy and survival in breast cancer: a systematic review and meta-analysis. BMC Cancer 13:240. doi:10.1186/1471-2407-13-240
Gagliato DDM, Gonzalez-Angulo AM, Lei X et al (2014) Clinical impact of delaying initiation of adjuvant chemotherapy in patients with breast cancer. J Clin Oncol 32:735–744. doi:10.1200/JCO.2013.49.7693
(2012) Guide for DoD researchers on using MHS data—guide for DoD researchers on using MHS data.pdf. http://www.tricare.mil/tma/privacy/hrpp/downloads/Guide for DoD researchers on using MHS data.pdf. Accessed 30 Aug 2014
Dignam JJ (2013) Hazard of recurrence among women after primary breast cancer treatment—a 10-year follow-up using data from SEER-medicare. Breast Dis A Year B Q 24:150–152. doi:10.1016/j.breastdis.2013.04.050
Cheng L, Swartz MD, Zhao H et al (2012) Hazard of recurrence among women after primary breast cancer treatment—a 10-year follow-up using data from SEER-medicare. Cancer Epidemiol Biomarkers Prev 21:800–809. doi:10.1158/1055-9965.EPI-11-1089
Chubak J, Yu O, Pocobelli G et al (2012) Administrative data algorithms to identify second breast cancer events following early-stage invasive breast cancer. J Natl Cancer Inst 104:931–940. doi:10.1093/jnci/djs233
Gallagher CM, More K, Masaquel A et al (2016) Survival in patients with non-metastatic breast cancer treated with adjuvant trastuzumab in clinical practice. SpringerPlus 5(1):1–10
Quan H, Sundararajan V, Halfon P et al (2005) Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care 43:1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
Elixhauser A, Steiner C, Kruzikas D (2004) HCUP methods series report # 2004-1
American Psychiatric Association, Inc (2013) Diagnostic and statistical manual of mental disorders: DSM-V. American Psychiatric Association, Inc, Toronto
(2014) The American College of Surgeons: National Accreditation Program for Breast Centers Standards Manual, pp 1–77
Howlader N, Chen VW, Ries LAG et al (2014) Overview of breast cancer collaborative stage data items—their definitions, quality, usage, and clinical implications: a review of SEER data for 2004-2010. Cancer 120(Suppl 23):3771–3780. doi:10.1002/cncr.29059
Acknowledgments
We would like to thank Ana Bozas, Ph.D., employee of Analysis Group Inc., for her contributions to the preparation and editing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
This study was funded by Genentech, Inc. Research data were derived from an approved Naval Medical Center, Portsmouth, VA IRB protocol. The views expressed in this study are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government. Drs. Gallagher and More were members of the U.S. Military at the time of the study. This work was prepared as part of their official duties. Title 17 U.S.C. 105 provides that ‘Copyright protection under this title is not available for any work of the United States Government.’ Title 17 U.S.C. 101 defines a United States Government work as a work prepared by a military service member or employee of the United States Government as part of that person’s official duties. T Kamath, A Masaquel, and B Barnett are employees of Genentech, Inc., and own stock/stock options. N Sicignano is an employee of Health ResearchTx, which has a business relationship with Genentech, Inc. A Guerin, R Ionescu-Ittu, M Gauthier-Loiselle, and E Wu are employees of Analysis Group Inc., which has received consultancy fees from Genentech, Inc. R Nitulescu was an employee of Analysis Group Inc. at the time when the study was conducted. Elizabeth Butts is an employee of the US Department of Defense and reports no financial interests.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Gallagher, C.M., More, K., Kamath, T. et al. Delay in initiation of adjuvant trastuzumab therapy leads to decreased overall survival and relapse-free survival in patients with HER2-positive non-metastatic breast cancer. Breast Cancer Res Treat 157, 145–156 (2016). https://doi.org/10.1007/s10549-016-3790-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-016-3790-3