
Abstract
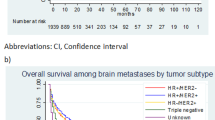
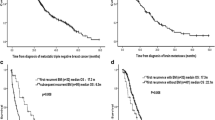
The incidences and clinical aggressiveness of intracranial metastases have not been as well characterized in patients with triple-negative (TN) breast cancer as in patients with human epidermal growth factor 2-positive (HER2+) breast cancer. Patients diagnosed with brain metastases from primary breast cancer, as determined by computed tomography and/or magnetic resonance imaging, at Asan Medical Center from January 1990 to July 2006 were identified and classified into three subtypes: TN, HER2+, and other. The clinical features and outcomes of these three groups were compared. Of the 7,872 patients diagnosed with primary breast cancer, 198 developed brain metastases; of these, 61 patients with unknown estrogen receptor, progesterone receptor, and HER2 status were excluded. Of the remaining 137 patients, 44 (32%) were classified as TN, 69 (50%) as HER2+, and 24 (18%) as other. Clinical parameters, including performance status and previous adjuvant chemotherapy and/or radiotherapy, were well balanced among groups, except that earlier staged tumors (I and II) were more prevalent in the TN than in the HER2+ and other (59 vs. 36 vs. 38%, P = 0.01). At a median follow-up of 99 months, the median times from initial diagnosis to brain metastasis (20 vs. 32 vs. 45 months, P = 0.01) and to first distant metastasis at any site (16 vs. 23 vs. 23 months, P = 0.005) were significantly shorter in TN than in the HER2+ and other. Median overall survival (OS) from primary cancer diagnosis was significantly shorter in the TN than in the HER2+ and other (31 vs. 39 vs. 57 months, P = 0.02), but survival after brain metastasis was similar (5.9 vs. 5.2 vs. 8.8 months, P = 0.31). Compared with other breast cancer phenotypes, TN breast cancer was characterized by earlier brain and other distant metastases and shorter OS, despite a higher proportion of tumors diagnosed at early stages.



Similar content being viewed by others

References
Perou CM, Sorlie T, Eisen MB et al (2000) Molecular portraits of human breast tumours. Nature 406:747–752
Nielsen TO, Hsu FD, Jensen K et al (2004) Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin Cancer Res 10:5367–5374
Reis-Filho JS, Tutt AN (2008) Triple negative tumours: a critical review. Histopathology 51:108–118
Irvin WJ Jr, Carey LA (2008) What is triple-negative breast cancer? Eur J Cancer 44:2799–2805
Sorlie T, Perou CM, Tibshirani R et al (2001) Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA 98:10869–10874
Foulkers WD, Brunet JS, Stefansson IM et al (2004) The prognostic implication of the basal-like (cyclin E high/p27 low/p53+/glomeruloid-microvascular-proliferation+) phenotype of BRCA1-related breast cancer. Cancer Res 64:830–835
Haffty BG, Yang Q, Reiss M et al (2006) Locoregional relapse and distant metastasis in conservatively managed triple negative early-stage breast cancer. J Clin Oncol 24:5652–5657
Di Sterano A, Yong Yap Y, Hortobagyi GN et al (1979) The natural history of breast cancer patients with brain metastases. Cancer 44:1913–1918
Fokstuen T, Wilking N, Rutqvist LE et al (2000) Radiation therapy in the management of brain metastases from breast cancer. Breast Cancer Res Treat 62:211–216
Lee SS, Ahn JH, Kim MK et al (2008) Brain metastases in breast cancer: prognostic factors and management. Breast Cancer Res Treat 111:523–530
Lin NU, Bellon JR, Winer EP (2004) CNS metastases in breast cancer. J Clin Oncol 22:3608–3617
Ryberg M, Nielsen D, Osterlind K et al (2005) Predictors of central nervous system metastasis in patients with metastatic breast cancer. A competing risk analysis of 579 patients treated with epirubicin-based chemotherapy. Breast Cancer Res Treat 91:217–225
Kirsch DG, Ledezma CJ, Mathews CS et al (2005) Survival after brain metastases from breast cancer in the trastuzumab era. J Clin Oncol 23:2114–2116
Bendell JC, Domchek SM, Burstein HJ et al (2003) Central nervous system metastases in women who receive trastuzumab-based therapy for metastatic breast cancer. Cancer 97:2972–2977
Church DN, Modgil R, Guglani S et al (2008) Extended survival in women with brain metastases from HER2 overexpressing breast cancer. Am J Clin Oncol 31:250–254
Park IH, Ro J, Lee KS et al (2009) Trastuzumab treatment beyond brain progression in HER2-positive metastatic breast cancer. Ann Oncol 20:56–62
Reiner A, Reiner G, Spona J et al (1998) Histopathologic characterization of human breast cancer in correlation with estrogen receptor status. A comparison of immunocytochemical and biochemical analysis. Cancer 15:1149–1154
Barnholtz-Sloan JS, Sloan AE, Davis FG et al (2004) Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol 22:2865–2872
Heitz F, Harter P, Lueck HJ et al (2009) Triple-negative and HER2-overexpressing breast cancers exhibit an elevated risk and an earlier occurrence of cerebral metastases. Eur J Cancer 45:2792–2798
Tham YL, Sexton K, Kramer R et al (2006) Primary breast cancer phenotypes associated with propensity for central nervous system metastases. Cancer 107:696–704
Nam BH, Kim SY, Han HS et al (2008) Breast cancer subtypes and survival in patients with brain metastases. Breast Cancer Res 10(1):R20. doi:10.1186/bcr1870
Niwinska A, Murawska M, Pogoda K (2010) Breast cancer brain metastases: differences in survival depending on biological subtype, RPA RTOG prognostic class and systemic treatment after whole-brain radiotherapy (WBRT). Ann Oncol 21:942–948
Kim MJ, Ro JY, Ahn SH et al (2006) Clinicopathologic significance of basal-like subtype of breast cancer: a comparison with hormone receptor and Her2/neu-overexpressing phenotypes. Hum Pathol 37:1217–1226
Hammond ME, Hayes DF, Dowsett M et al (2010) American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol 28:2784–2795
Harvey JM, Clark GM, Osborne CK, Allred DC (1999) Estrogen receptor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapy in breast cancer. J Clin Oncol 17:1474–1481
Eichler AF, Kuter I, Ryan P et al (2008) Survival in patients with brain metastases from breast cancer: the importance of HER-2 status. Cancer 112:459–469
Pienkowski T, Zielinski CC (2010) Trastuzumab treatment in patients with breast cancer and metastatic CNS disease. Ann Oncol 21:917–924
Clayton AJ, Danson S, Jolly S et al (2004) Incidence of cerebral metastases in patients treated with trastuzumab for metastatic breast cancer. Br J Cancer 91:639–643
Miller KD, Weathers T, Haney LG et al (2003) Occult central nervous system involvement in patients with metastatic breast cancer: prevalence, predictive factors and impact on survival. Ann Oncol 14:1072–1077
Melisko ME, Glantz M, Rugo HS (2009) New challenges and opportunities in the management of brain metastases in patients with ErbB2-positive metastatic breast cancer. Nat Clin Pract Oncol 6:25–33
Lin NU, Winer EP (2007) Brain metastases: the HER2 paradigm. Clin Cancer Res 13:1648–1655
Geyer CE, Forster J, Lindquist D et al (2006) Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med 28:2733–2743
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jang, G., Lee, S.S., Ahn, JH. et al. Clinical features and course of brain metastases in triple-negative breast cancer: comparison with human epidermal growth factor receptor 2-positive and other type at single institution in Korea. Breast Cancer Res Treat 128, 171–177 (2011). https://doi.org/10.1007/s10549-011-1526-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-011-1526-y