
Abstract
Purpose
This study aimed to compare the combination of a lateral femoral cutaneous nerve (LFCN) block with a femoral nerve block (FNB) and an adductor canal block (ACB) for postoperative pain control in patients undergoing anterior cruciate ligament (ACL) reconstruction with hamstring autograft.
Methods
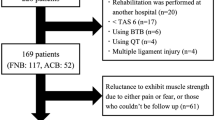
A non-randomized, prospective, controlled clinical trial was conducted. The FNB and ACB groups consisted of 41 and 40 patients, respectively. Thirty minutes prior to surgery, the patients received an ultrasound-guided LFCN block either with FNB or ACB. The following values were recorded and compared between the two groups: duration of surgery, pain management during surgery (including total amount of fentanyl administered), and numerical rating scale (NRS) scores at 30 min and 4, 8, 12, 24, 48, and 72 h after surgery. Factors affecting pain relief (NRS < 2) were evaluated, including block type, total amount of fentanyl administered, duration of surgery, age, sex, body mass index, and postoperative suppository use. Significant factors predicting pain relief were determined using the Cox proportional hazard regression model.
Results
There were no significant differences in pain management during the surgery. Pain scores were significantly lower in the ACB group at 30 min, 4 h, 24 h, and 48 h after surgery. The Cox proportional hazard regression model identified ACB as a significant factor for pain relief (hazard ratio: 1.88; 95% confidence interval: 1.12–3.13; p = 0.018).
Conclusion
The combination of ACB with LFCN block during ACL reconstruction significantly reduced pain in the early postoperative period compared to FNB with LFCN block.




Similar content being viewed by others


Data availability
The data that support the findings of this study are available on request from the corresponding author, JN. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
References
Cohn BT, Draeger RI, Jackson DW. The effects of cold therapy in the postoperative management of pain in patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med. 1989;17:344–9.
Alford JW, Fadale PD. Evaluation of postoperative bupivacaine infusion for pain management after anterior cruciate ligament reconstruction. Arthrosc J Arthrosc Relat Surg. 2003;19:855–61.
Beck PR, Nho SJ, Balin J, et al. Postoperative pain management after anterior cruciate ligament reconstruction. J Knee Surg. 2004;17:18–23.
Kocher MS, Steadman JR, Briggs K, et al. Determinants of patient satisfaction with outcome after anterior cruciate ligament reconstruction. J Bone Jt Surg Ser A. 2002;84:1560–72.
Secrist ES, Freedman KB, Ciccotti MG, et al. Pain management after outpatient anterior cruciate ligament reconstruction: a systematic review of randomized controlled trials. Am J Sports Med. 2016;44:2435–47.
Williams BA, Kentor ML, Vogt MT, et al. Economics of nerve block pain management after anterior cruciate ligament reconstruction. Anesthesiology. 2004;100:697–706.
Akinci SB, Saricaoǧlu F, Atay OA, et al. Analgesic effect of intra-articular tramadol compared with morphine after arthroscopic knee surgery. Arthrosc J Arthrosc Relat Surg. 2005;21:1060–5.
Mayr HO, Entholzner E, Hube R, et al. Pre-versus postoperative intraarticular application of local anesthetics and opioids versus femoral nerve block in anterior cruciate ligament repair. Arch Orthop Trauma Surg. 2007;127:241–4.
Kurosaka K, Tsukada S, Nakayama H, et al. Periarticular injection versus femoral nerve block for pain relief after anterior cruciate ligament reconstruction: a randomized controlled trial. Arthrosc J Arthrosc Relat Surg. 2018;34:182–8.
Kristensen PK, Pfeiffer-Jensen M, Storm JO, et al. Local infiltration analgesia is comparable to femoral nerve block after anterior cruciate ligament reconstruction with hamstring tendon graft: A randomised controlled trial. Knee Surg Sports Traumatol Arthrosc. 2014;22:317–23.
Nakase J, Shimozaki K, Asai K, et al. Usefulness of lateral femoral cutaneous nerve block in combination with femoral nerve block for anterior cruciate ligament reconstruction: a prospective trial. Arch Orthop Trauma Surg. 2021;141:455–60.
Ogura T, Omatsu H, Fukuda H, et al. Femoral nerve versus adductor canal block for early postoperative pain control and knee function after anterior cruciate ligament reconstruction with hamstring autografts: a prospective single-blind randomised controlled trial. Arch Orthop Trauma Surg. 2021;141:1927–34.
Lynch JR, Okoroha KR, Lizzio V, et al. Adductor canal block versus femoral nerve block for pain control after anterior cruciate ligament reconstruction: a prospective randomized trial. Am J Sports Med. 2019;47:355–63.
Mall NA, Wright RW. Femoral nerve block use in anterior cruciate ligament reconstruction surgery. Arthrosc J Arthrosc Relat Surg. 2010;26:404–16.
Nielsen TD, Moriggl B, Barckman J, et al. The lateral femoral cutaneous nerve: description of the sensory territory and a novel ultrasound-guided nerve block technique. Reg Anesth Pain Med. 2018;43:357–66.
Nakase J, Toratani T, Kosaka M, et al. Technique of anatomical single bundle ACL reconstruction with rounded rectangle femoral dilator. Knee. 2016;23:91–6.
Kwofie MK, Shastri UD, Gadsden JC, et al. The effects of ultrasound-guided adductor canal block versus femoral nerve block on quadriceps strength and fall risk. Reg Anesth Pain Med. 2013;38:321–5.
Wong WY, Bjørn S, Strid JMC, et al. Defining the location of the adductor canal using ultrasound. Reg Anesth Pain Med. 2017;42:241–5.
Manickam B, Perlas A, Duggan E, et al. Feasibility and efficacy of ultrasound-guided block of the saphenous nerve in the adductor canal. Reg Anesth Pain Med. 2009;34:578–80.
Vilhelmsen F, Nersesjan M, Andersen JH, et al. Lateral femoral cutaneous nerve block with different volumes of Ropivacaine: A randomized trial in healthy volunteers. BMC Anesthesiol. 2019;19:1–8.
Ghodki PS, Shalu PS, Sardesai SP. Ultrasound-guided adductor canal block versus femoral nerve block for arthroscopic anterior cruciate ligament repair under general anesthesia. J Anaesthesiol Clin Pharmacol. 2018;34:242–6.
Beck P, Nho S, Balin J, et al. Postoperative pain management after anterior cruciate ligament reconstruction. J Knee Surg. 2010;17:18–23.
Dauri M, Fabbi E, Mariani P, et al. Continuous femoral nerve block provides superior analgesia compared with continuous intra-articular and wound infusion after anterior cruciate ligament reconstruction. Reg Anesth Pain Med. 2009;34:95–9.
Dauri M, Polzoni M, Fabbi E, et al. Comparison of epidural, continuous femoral block and intraarticular analgesia after anterior cruciate ligament reconstruction. Acta Anaesthesiol Scand. 2003;47:20–5.
Frost S, Grossfeld S, Kirkley A, et al. The efficacy of femoral nerve block in pain reduction for outpatient hamstring anterior cruciate ligament reconstruction: A double-blind, prospective, randomized trial. Arthroscopy. 2000;16:243–8.
Guirro UBDP, Tambara EM, Munhoz FR. Femoral nerve block: Assessment of postoperative analgesia in arthroscopic anterior cruciate ligament reconstruction. Brazilian J Anesthesiol. 2013;63:483–91.
Luo TD, Ashraf A, Dahm DL, et al. Femoral nerve block is associated with persistent strength deficits at 6 months after anterior cruciate ligament reconstruction in pediatric and adolescent patients. Am J Sports Med. 2015;43:331–6.
Christensen JJ, Krych AJ, Engasser WM, et al. Lateral tibial posterior slope is increased in patients with early graft failure after anterior cruciate ligament reconstruction. Am J Sports Med. 2015;43:2510–4.
Magnussen RA, Pottkotter K, Di SS, et al. Femoral nerve block after anterior cruciate ligament reconstruction. J Knee Surg. 2017;30:323–8.
Petersen W, Taheri P, Forkel P, et al. Return to play following ACL reconstruction: a systematic review about strength deficits. Arch Orthop Trauma Surg. 2014;134:1417–28.
Jæger P, Nielsen ZJK, Henningsen MH, et al. Adductor canal block versus femoral nerve block and quadriceps strength. Anesthesiology. 2013;118:409–15.
Abdallah FW, Whelan DB, Chan VW, et al. Adductor canal block provides noninferior analgesia and superior quadriceps strength compared with femoral nerve block in anterior cruciate ligament reconstruction. Anesthesiology. 2016;124:1053–64.
Bailey L, Griffin J, Elliott M, et al. Adductor canal nerve versus femoral nerve blockade for pain control and quadriceps function following anterior cruciate ligament reconstruction with patellar tendon autograft: a prospective randomized trial. Arthrosc J Arthrosc Relat Surg. 2019;35:921–9.
Runner RP, Boden SA, Godfrey WS, et al. Quadriceps strength deficits after a femoral nerve block versus adductor canal block for anterior cruciate ligament reconstruction: a prospective, single-blinded. Randomiz Trial Orthop J Sport Med. 2018;6:1–8.
Edwards MD, Bethea JP, Hunnicutt JL, et al. Effect of adductor canal block versus femoral nerve block on quadriceps strength, function, and postoperative pain after anterior cruciate ligament reconstruction: a systematic review of level 1 studies. Am J Sports Med. 2020;48:2305–13.
Christensen JE, Taylor NE, Hetzel SJ, et al. Isokinetic strength deficit 6 months after adductor canal blockade for anterior cruciate ligament reconstruction. Orthop J Sport Med. 2017;5:1–6.
Lonchena TK, McFadden K, Orebaugh SL. Correlation of ultrasound appearance, gross anatomy, and histology of the femoral nerve at the femoral triangle. Surg Radiol Anat. 2016;38:115–22.
Ritter JW. Femoral nerve “sheath” for inguinal paravascular lumbar plexus block is not found in human cadavers. J Clin Anesth. 1995;7:470–3.
Tubbs RS, Loukas M, Shoja MM, et al. Anatomy and potential clinical significance of the vastoadductor membrane. Surg Radiol Anat. 2007;29:569–73.
Elazab E. Subsartorial compartments and membranes in the adductor canal:morphological, histological and Immunohistochemical Study. Egypt J Anat. 2017;40:1–17.
Goffin P, Lecoq JP, Ninane V, et al. Interfascial spread of injectate after adductor canal injection in fresh human cadavers. Anesth Analg. 2016;123:501–3.
Runge C, Moriggl B, Børglum J, et al. The spread of ultrasound-guided injectate from the adductor canal to the genicular branch of the posterior obturator nerve and the popliteal plexus: a cadaveric study. Reg Anesth Pain Med. 2017;42:725–30.
Funding
This study received no funding.
Author information
Authors and Affiliations
Contributions
Conceptualization: JN. Project administration and supervision: JN and HT. Investigation, formal analysis, and validation: TO, YI, and YY. Writing-original draft: TO. Writing-review and editing: JN, TK, and HT.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical approval
The study design was prospectively reviewed and approved by our institutional ethics committee (1842–3).
Consent to publish
Participants provided written consent for publication of images.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Oshima, T., Nakase, J., Kanayama, T. et al. Ultrasound-guided adductor canal block is superior to femoral nerve block for early postoperative pain relief after single-bundle anterior cruciate ligament reconstruction with hamstring autograft. J Med Ultrasonics 50, 433–439 (2023). https://doi.org/10.1007/s10396-023-01309-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10396-023-01309-8