
Abstract
Background
Carotid and brachial artery intima-media thicknesses (IMT) determined using B-mode ultrasonography are validated surrogate markers of the severity and extent of coronary artery disease (CAD). The markers may also reflect the general vascular atherosclerotic involvement and cardiovascular risk in patients with normal coronary arteries (NCA). We aimed to investigate the relationship of carotid artery IMT (CIMT) and brachial artery IMT (BIMT) with CAD simultaneously, and also examined whether both markers represent cardiovascular risk determined by cardiovascular risk factors in patients with NCA.
Methods
One hundred eligible patients who consecutively underwent coronary angiography under suspicion of CAD were included in this study. The patients were evaluated in terms of age, gender, and the risk factors for CAD, and their total cardiovascular risk was calculated. CIMT and BIMT measurements were performed by B-mode ultrasonography on all patients. The extent and severity of CAD were evaluated by the Gensini score, and the number of severely narrowed vessels was determined by coronary angiography.
Results
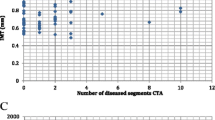
Sixty-three patients (47 males, 16 females) with a mean age of 62 ± 10 years had CAD, and 37 patients (20 males, 17 females) with a mean age of 51 ± 11 years had NCA on coronary angiography. The mean age and male ratio of patients with CAD were significantly higher as compared with the patients with NCA (p < 0.001, p = 0.035, respectively). The mean number of diseased vessels was 2.2 ± 0.9 (median 2.0), while the mean Gensini score was 25 ± 31 (median 14.0). The CIMT and BIMT were higher in patients with CAD than in those with NCA (0.9 ± 0.2 vs. 0.7 ± 0.2 mm and 0.5 ± 0.1 vs. 0.4 ± 0.1 mm, respectively; p < 0.001 for both). The cardiovascular risk score (CVRS) was also significantly higher in the CAD group (3.8 ± 1.1 vs. 2.9 ± 1.4, p < 0.001). CIMT, BIMT, and CVRS were significantly correlated with the Gensini score and number of diseased vessels. For the sensitivity and the specificity of CIMT, BIMT, and CVRS to detect the presence of CAD, the areas under the ROC curve were 0.785 (95% CI 0.687–0.883, p = 0.000), 0.842 (95% CI 0.764–0.920, p = 0.000), and 0.721 (95% CI 0.591–0.813, p = 0.001), respectively. When we compared the CVRSs between the groups, which were determined according to cutoff values for CIMT and BIMT (CIMT ≥0.9 vs. <0.9 and BIMT ≥0.4 vs. <0.4); among the patients with NCA, CVRSs were significantly different (3.5 ± 0.5 vs. 2.7 ± 1.4, p = 0.035 and 3.7 ± 1.1 and 2.7 ± 1.3, p = 0.073; respectively).
Conclusion
The increases in both brachial and carotid IMT are positively correlated with the extent of CAD and the number of involved vessels, and have more predictive value for CAD than the traditional CVRS. In addition, carotid IMT is also related to high CVRS in patients with NCA, and this finding may represent general vascular involvement without coronary lesions determined by coronary angiography.

Similar content being viewed by others


References
Adams MR, Nakagomi A, Keech A, Robinson J, McCredie R, Bailey BP, Freedman SB, Celermajer DS. Carotid intima-media thickness is only weakly correlated with the extent and severity of coronary artery disease. Circulation. 1995;92:2127–34.
Craven TE, Ryu JE, Espeland MA, Kahl FR, McKinney WM, Toole JF, McMahan MR, Thompson CJ, Heiss G, Crouse JR 3rd. Evaluation of the association between carotid artery atherosclerosis and coronary artery stenosis. Circulation. 1990;82:1230–42.
Howard G, Sharrett AR, Heiss G, Evans GW, Chambless LE, Riley WA, Burke GL. Carotid artery intimal-medial thickness distribution in general populations as evaluated by B-mode ultrasound. Stroke. 1993;24:1297–304.
Kitamura A, Iso H, Imano H, Ohira T, Sato S, Naito Y, Iida M, Shimamoto T. Prevalence and correlates of carotid atherosclerosis among elderly Japanese men. Atherosclerosis. 2004;172:353–9.
Bots ML, Hoes AW, Koudstall PS, Hofman A, Grobbee DE. Common carotid intima-media thickness and risk of stroke and myocardial infarction. The Rotterdam study. Circulation. 1997;96:1432–7.
O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK Jr. Carotid artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. N Engl J Med. 1999;340:14–22.
Gensini GG. Coronary angiography. Mount Kisco: Futura Publishing Co; 1975.
Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, Najjar SS, Rembold CM, Post WS. American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. 2008;21(2):93–111 (quiz 189-90).
Guidelines Committee 2003 European Society of Hypertension. European Society of Cardiology guidelines for the management of hypertension. J Hypertens. 2003;21:1011–1053.
Korkmaz H, Akbulut M, Ozbay Y, Koç M. The relation of intima-media thickness with endothelial function and left ventricular mass index (brachial artery intima-media thickness). Anadolu Kardiyol Derg. 2010;10:220–5.
Lind L, Andersson J, Rönn M, Gustavsson T, Holdfelt P, Hulthe J, Elmgren A, Zilmer K, Zilmer M. Brachial artery intima-media thickness and echogenicity in relation to lipids and markers of oxidative stress in elderly subjects—The Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) Study. Lipids. 2008;43:133–41.
Crouse JR, Craven TE, Hagaman AP, Bond G. Association of coronary disease with segment-specific intimal-medial thickening of the extracranial carotid artery. Circulation. 1995;92:1141–7.
Hulthe J, Wikstrand J, Emanuelson H, Wiklund O, de Feyter PJ, Wendelhag I. Atherosclerotic changes in the carotid artery bulb as measured by B-mode ultrasound are associated with the extent of coronary atherosclerosis. Stroke. 1997;28:1189–94.
Lekakis JP, Papamichael C, Papaioannou TG, Stamatelopoulos KS, Cimponeriu A, Protogerou AD, Kanakakis J, Stamatelopoulos SF. Intima-media thickness score from carotid and femoral arteries predicts the extent of coronary artery disease. Int J Cardiovasc Imag. 2005;21:495–501.
Bonithon-Kopp C, Scarabin P, Taquet A, Touboul P, Malnejak A, Guize L. Risk factors for early carotid atherosclerosis in middle-aged French women. Arterioscler Thromb. 1991;11:966–972.
Sutton-Tyrrell K, Lassila HC, Meilahn E, Bunker C, Matthews KA, Kuller LH. Carotid atherosclerosis in postmenopausal women and its association with risk factors measured after menopause. Stroke. 1998;29:1116–21.
Chambless LE, Heiss G, Folsom AR, Rosamond W, Szklo M, Sharrett AR, Clegg LX. Association of coronary heart disease incidence with carotid arterial wall 501 thickness and major risk factors: the Atherosclerosis Risk in Communities (ARIC) Study, 1987–1993. Am J Epidemiol. 1997;146:483–94.
Bard RL, Kalsi H, Rubenfire M, Wakefield T, Fex B, Rajagopalan S, Brook RD. Effect of carotid atherosclerosis screening on risk stratification during primary cardiovascular disease prevention. Am J Cardiol. 2004;93:1030–2.
Hodis HN, Mack WJ, LaBree L, Selzer RH, Liu CR, Liu CH, Azen SP. The role of carotid artery intima-media thickness in predicting clinical coronary events. Ann Intern Med. 1998;128:262–9.
Pignoli P, Tremoli E, Poli A, Oreste P, Paoletti R. Intimal plus medial thickness of the arterial wall: a direct measurement with ultrasound imaging. Circulation. 1986;7:1399–406.
Persson J, Formgren J, Israelsson B, Berglund G. Ultrasound-determined intima-media thickness and atherosclerosis. Direct and indirect validation. Arterioscler Thrornb. 7994;14:261–4.
Geroulakos G, O’Gorman DJ, Kalodiki E, Sheridan DJ, Nicolaides AN. The carotid intima-media thickness as a marker of the presence of severe symptomatic coronary artery disease. Eur Heart J. 1994;15:781–5.
Salonen JT, Seppänen K, Rauramaa R, Salonen R. Risk factors for carotid atherosclerosis: the Kuopio Ischaemic Heart Disease Risk Factor Study. Ann Med. 1989;21:227–9.
Salonen JT, Salonen R. Ultrasound B-mode imaging in observational studies of atherosclerotic progression. Circulation. 1993;87(suppl):Il-56–II-65.
Belcaro G, Nicolaides AN, Laurora G, Cesarone MR, De Sanctis M, Incandela L, Barsotti A. Ultrasotind morphology classiflcation of the arterial wall and cardiovascular events in a 6-year follow-up study. Arterioscler Thromb Vasc BİoI. 1996;16:851–6.
Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. Common carotid intima-media thickness and risk of stroke and myocardial infarction: the Rotterdam study. Circulation. 1997;96:1432–7.
Crouse JR III, Byington RP, Bond MG, Espeland MA, Craven TE, Sprinkle JW, McGovern ME, Furberg CD. Pravastatin, lipids, and atherosclerosis in the carotid arteries (PLAC-ll). Am J Cardiol. 1995;75:455–9.
Crouse JR III, Raichlen JS, Riley WA, Evans GW, palmer MK, O’Leary DH, Grobbee DE, Bots ML, METEOR Study Group. Effect of rosuvastatin on progression of carotid intima-media thickness in low-risk individuals with subclinical atherosclerosis: the METEOR trial. JAMA. 2007;297:1344–1353.
Salonen R, Salonen JT. Progression of carotid atherosclerosis and its determinants: a population-based ultrasonography study. Atherosclerosis. 1990;81:33–40.
Steven J, Lester SJ, Eleid MF, Khandheria BK, Hurst RT. Carotid intima-media thickness and coronary artery calcium score as indications of subclinical atherosclerosis. Mayo Clin Proc. 2009;84:229–33.
Holewijn S, Heijer M, Stalenhoef AF, Graaf J. Non-invasive measurements of atherosclerosis (NI MA): current evidence and future perspectives. Netherlands J Med. 2010;68:388–99.
Kawamoto R, Tomita H, Ohtsuka N, Inoue A, Kamitani A. Metabolic syndrome, diabetes and subclinical atherosclerosis as assessed by carotid intima-media thickness. J Atheroscler Thromb. 2007;14:78–85.
Pollex RL, Al-Shali KZ, House AA, Spence JD, Fenster A, Mamakeesick M, Zinman B, Harris SB, Hanley AJ, Hegele RA. Relationship of the metabolic syndrome to carotid ultrasound traits. Cardiovasc Ultrasound. 2006;7:4–28.
Arroyo-Espliguero R, Mollichelli N, Avanzas P, Zouridakis E, Newey VR, Nassiri DK, Kaski JC. Chronic inflammation and increased arterial stiffness in patients with cardiac syndrome X. Eur Heart J. 2003;24:2006–11.
Cho SH, Jeong MH, Park IH, Choi JS, Yoon HJ, Kim KH, Hong YJ, Park HW, Kim JH, Ahn Y, Cho JG, Park JC, Kang JC. Endothelial dysfunction, increased carotid artery intima-media thickness and pulse wave velocity, and increased level of inflammatory markers are associated with variant angina. J Cardiol. 2009;54:183–91.
Poyet R, Cuisset T, Bali L, Quilici J, Lambert M, Bonnet JL. Coronary wall characteristics after myocardial infarction without significant coronary angiographic lesion: an intravascular ultrasound study. Acta Cardiol. 2010;65:627–30.
Wu YW, Chen YH, Wang SS, Jui HY, Yen RF, Tzen KY, Chen MF, Lee CM. PET assessment of myocardial perfusion reserve inversely correlates with intravascular ultrasound findings in angiographically normal cardiac transplant recipients. J Nucl Med. 2010;51:906–12.
Khuddus MA, Pepine CJ, Handberg EM, Bairey Merz CN, Sopko G, Bavry AA, Denardo SJ, McGorray SP, Smith KM, Sharaf BL, Nicholls SJ, Nissen SE, Anderson RD. An intravascular ultrasound analysis in women experiencing chest pain in the absence of obstructive coronary artery disease: a substudy from the National Heart, Lung and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation (WISE). J Interv Cardiol. 2010;23:511–9.
Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, Najjar SS, Rembold CM, Post WS. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force: endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. 2008;21:376.
Conflict of interest
None of the authors has a conflict of interest to report.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Şatiroğlu, Ö., Kocaman, S.A., Bayar, N. et al. Carotid and brachial artery intima-media thickness is related to coronary atherosclerotic burden and may also represent high cardiovascular risk in patients with normal coronary angiograms. J Med Ultrasonics 38, 187–194 (2011). https://doi.org/10.1007/s10396-011-0319-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10396-011-0319-6