
Abstract
Purpose
Asymmetric dilated vortex vein (ADVV) observed in eyes with pachychoroid spectrum diseases is thought to be due to congestion of choroidal blood flow. The purpose of this study was to quantitatively investigate the blood flow velocity of ADVV using laser speckle flowgraphy (LSFG).
Study design
Retrospective case series.
Methods
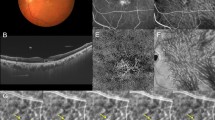
This was a retrospective case series with 23 eyes of 18 patients with ADVV on en-face OCT. A pair of choroidal veins from ADVV side (defined as ADVV vein) and non-ADVV side (defined as non-ADVV vein) was selected in each eye under the following criteria: (i) equivalent proximity to the deviated watershed, (ii) does not overlap with retinal blood vessels in the en-face OCT image, (iii) has approximately the same blood vessel diameter. Rubber bands were placed on the selected choroidal veins on the LSFG color map. Mean blur rate (MBR) values of ADVV and non-ADVV veins were statistically compared.
Results
The average MBR was 10.11 ± 1.9 in the ADVV veins and 13.49 ± 6.2 in the non-ADVV veins, showing significantly lower values in the ADVV veins (P = 0.03). The blood vessel diameter of the ADVV was 10.26 ± 3.0 and in the non-ADVV veins, 10.63 ± 2.9 pixels; not significantly different (P = 0.66). The distance from the deviated watershed to the ADVV was 53.3 ± 24.8 and to the non-ADVV veins, 46.80 ± 20.3 pixels; not significantly different (P = 0.41).
Conclusion
In eyes with ADVV, the blood flow velocity in the ADVV veins was lower than in the non-ADVV veins, suggesting anatomical congestion of ADVV.



Similar content being viewed by others


References
Guyer DR, Yannuzzi LA, Slakter JS, Sorenson JA, Ho A, Orlock D. Digital indocyanine green videoangiography of central serous chorioretinopathy. Arch Ophthalmol. 1994;112:1057–62.
Imamura Y, Fujiwara T, Margolis R, Spaide RF. Enhanced depth imaging optical coherence tomography of the choroid in central serous chorioretinopathy. Retina. 2009;29:1469–73.
Hiroe T, Kishi S. Dilatation of asymmetric vortex vein in central serous chorioretinopathy. Ophthalmol Retina. 2018;2:152–61.
Saito M, Saito W, Hashimoto Y, Yoshizawa C, Fujiya A, Noda K, et al. Macular choroidal blood flow velocity decreases with regression of acute central serous chorioretinopathy. Br J Ophthalmol. 2013;97:775–80.
Saito M, Saito W, Hirooka K, Hashimoto Y, Mori S, Noda K, et al. Pulse waveform changes in macular choroidal hemodynamics with regression of acute central serous chorioretinopathy. Invest Ophthalmol Vis Sci. 2015;56:6515–22.
Imanaga N, Terao N, Nakamine S, Tamashiro T, Wakugawa S, Sawaguchi K, et al. Scleral thickness in central serous chorioretinopathy. Ophthalmol Retina. 2021;5:285–91.
Terao N, Koizumi H, Kojima K, Kusada N, Nagata K, Yamagishi T, et al. Short axial length and hyperopic refractive error are risk factors of central serous chorioretinopathy. Br J Ophthalmol. 2020;104:1260–5.
Ersoz MG, Arf S, Hocaoglu M, Sayman Muslubas I, Karacorlu M. Patient characteristics and risk factors for central serous chorioretinopathy: an analysis of 811 patients. Br J Ophthalmol. 2019;103:725–9.
Cardillo Piccolino F, Lupidi M, Cagini C, Fruttini D, Nicolò M, et al. Choroidal vascular reactivity in central serous chorioretinopathy. Invest Ophthalmol Vis Sci. 2018;59:3897–905.
Sun J, Tan J, Wang Z, Yang H, Zhu X, Li L. Effect of catecholamine on central serous chorioretinopathy. J Huazhong Univ Sci Technol Med Sci. 2003;23:313–6.
Islam QU, Hanif MK, Tareen S. Frequency of systemic risk factors in central serous chorioretinopathy. J Coll Phys Surg Pak. 2016;26:692–5.
Liu B, Deng T, Zhang J. Risk factors for central serous chorioretinopathy: a systematic review and meta-analysis. Retina. 2016;36:9–19.
Venkatesh P, Gadia R, Tewari HK, Kumar D, Garg S. Prehypertension may be common in patients with central serous choroioretinopathy. Graefes Arch Clin Exp Ophthalmol. 2006;244:1101–3.
Saito M, Noda K, Saito W, Hirooka K, Hashimoto Y, Ishida S. Increased choroidal blood flow and choroidal thickness in patients with hypertensive chorioretinopathy. Graefes Arch Clin Exp Ophthalmol. 2020;258:233–40.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
K. Hirooka, None; M. Saito, None; Y. Yamashita, None; Y. Hashimoto, None; N. Terao, None; H. Koizumi, None; K. Noda, None; S. Ishida, None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Corresponding Author: Michiyuki Saito
Supplementary Information
Below is the link to the electronic supplementary material.
10384_2021_889_MOESM1_ESM.tif
Supplemental Figure 1. Schema Showing the Pathology of Pachychoroid as Choroidal Congestion and Hyperperfusion. The faucet represents the choroidal artery, the drainage hole represents the vortex vein, and the water in the bathtub represents the total lumen of the choroidal vasculature. (a) Normal choroid: Water is flowing into a bathtub with an open hole, and the amount of water in this bathtub is in equilibrium with a good balance between inflow and outflow. (b) Uncomplicated pachychoroid: When the drainage hole is narrowed (congestion), the balance between inflow and drainage is lost and the water level rises (choroidal vessel dilation followed by choroidal thickening), and due to the increased hydrostatic pressure, a new equilibrium state is achieved at the elevated water level as the disturbed outflow catches up to inflow. (c) The pathogenesis of CSC: When the faucet is potently opens to increase the amount of inflowing water (hyperperfusion), the balance between inflow and drainage is further lost, the water level rises beyond the capacity of the bathtub showing overflow (choroidal vascular hyperpermeability followed by subretinal fluid accumulation) (TIF 254 kb)
About this article

Cite this article
Hirooka, K., Saito, M., Yamashita, Y. et al. Imbalanced choroidal circulation in eyes with asymmetric dilated vortex vein. Jpn J Ophthalmol 66, 14–18 (2022). https://doi.org/10.1007/s10384-021-00889-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10384-021-00889-7