
Abstract
Purpose
The standard management of rectal cancer continues to be defined by the results of randomized, clinical trials exploring the optimal timing and use of adjuvant chemotherapy and radiation therapy in relation to surgery. The patient with rectal cancer who is elderly and/or has significant comorbidities and the patient who refuses surgery are clinical contexts for which there is limited current data to guide decision making.
Methods
A retrospective analysis was performed at six Australian centers of patients with rectal cancer treated with radiation therapy or chemoradiation alone because of excessive operative risk or patient refusal of surgery.
Results
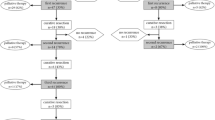
We identified 48 patients treated between August 1998 and June 2005 with a median age of 76 (range, 49–94) years. Twenty-four patients (50 percent) were considered medically inoperable and 24 patients refused surgery. Treatment was with chemoradiation (with 5-fluorouracil) in 36 patients and radiotherapy alone in 12 patients; 93 percent completed the planned therapy. A clinical complete response was seen in 56 percent and a partial response in 30 percent of patients. At a median follow-up of 49 months, 18 patients have disease progression, including 10 of 24 in the medically inoperable group and 8 of 24 in the refused surgery group. Of the 25 deceased patients, 16 died from progressive disease and 9 from noncancer causes.
Conclusions
Chemoradiation or radiotherapy alone is a safe alternative that results in significant progression-free and overall survival times in patients who are considered medically inoperable or refuse to undergo surgery. Ultimately, however, many patients will progress.



Similar content being viewed by others

References
Colorectal Cancer Collaborative Group. Adjuvant radiotherapy for rectal cancer: a systematic overview of 8,507 patients from 22 randomized trials. Lancet 2001;358:1291–304
Habr-Gama A, de Souza PM, Ribeiro U Jr, et al. Low rectal cancer: impact of radiation and chemotherapy on surgical treatment. Dis Colon Rectum 1998;41:1087–96
Luna-Perez P, Rodriguez-Ramirez S, Rodriguez-Coria DF, et al. Preoperative chemoradiation therapy and anal sphincter preservation with locally advanced rectal adenocarcinoma. World J Surg 2001;25:1006–11.
Medich D, McGinty J, Parda D, et al. Preoperative chemoradiotherapy and radical surgery for locally advanced distal rectal adenocarcinoma: pathologic findings and clinical implications. Dis Colon Rectum 2001;44:1123–8.
Grann A, Minsky BD, Cohen AM, et al. Preliminary results of preoperative 5-fluorouracil, low-dose leucovorin, and concurrent radiation therapy for clinically resectable T3 rectal cancer. Dis Colon Rectum 1997;40:515–22.
Janjan NA, Khoo VS, Abbruzzese J, et al. Tumor downstaging and sphincter preservation with preoperative chemoradiation in locally advanced rectal cancer: the M. D. Anderson Cancer Center experience. Int J Radiat Oncol Biol Phys 1999;44:1027–38.
Hiotis SP, Weber SM, Cohen AM, et al. Assessing the predictive value of clinical complete response to neoadjuvant therapy for rectal cancer: an analysis of 488 patients. J Am Coll Surg 2002;194:131–5.
Habr-Gama A, Perez RO, Nadalin W, et al. Long-term results of preoperative chemoradiation for distal rectal cancer correlation between final stage and survival. J Gastrointest Surg 2005;1:90–9.
Ruo L, Tickoo S, Klimstra DS, et al. Long-term prognostic significance of extent of rectal cancer response to preoperative radiation and chemotherapy. Ann Surg 2002;236:75–81.
Garcia-Aguilar J, Hernandez de Anda E, Sirivongs P, et al. A pathologic complete response to preoperative chemoradiation is associated with lower local recurrence and improved survival in rectal cancer patients treated by mesorectal excision. Dis Colon Rectum 2003;46:298–304.
Habr-Gama A, Perez RO, Nadalin W, et al. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy. Long-term results. Ann Surg 2004;240:711–8.
Luna-Perez P, Rodriguez-Ramirez S, Vega J, et al. Morbidity and mortality following abdominoperineal resection for low rectal adenocarcinoma. Rev Invest Clin 2001;53:388–95.
Wang Y, Cummings B, Catton P, et al. Primary radical external beam radiotherapy of rectal adenocarcinoma: long-term outcome of 271 patients. Radiother Oncol 2005;77:126–32.
Gerard JP, Chapet O, Ramaioli A, Romestaing P. Long-term control of T2-T3 rectal adenocarcinoma with radiotherapy alone. Int J Radiat Oncol Biol Phys 2002;54:142–9.
Rossi BM, Nakagawa WT, Novaes PE, Filho WD, Lopes A. Radiation and chemotherapy instead of surgery for low infiltrative rectal adenocarcinoma: a prospective trial. Ann Surg Oncol 1998;5:113–8.
Nakagawa WT, Rossi BM, Ferreira FD, et al. Chemoradiation instead of surgery to treat mid and low rectal tumors: is it safe? Ann Surg Oncol 2003;9:568–73
Moore H, Gittleman A, Minsky B, et al. Rate of pathologic complete response with increased interval between preoperative combined modality therapy and rectal cancer resection. Dis Colon Rectum 2004;47:279–86.
Vather R, Zargar-Shoshtari K, Adegbola S, Hill AG. Comparison of the possum, P-POSSUM and Cr-POSSUM scoring systems as predictors of postoperative mortality in patients undergoing major colorectal surgery. ANZ J Surg 2006;76:812–6.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Lim, L., Chao, M., Shapiro, J. et al. Long-Term Outcomes of Patients with Localized Rectal Cancer Treated with Chemoradiation or Radiotherapy Alone Because of Medical Inoperability or Patient Refusal. Dis Colon Rectum 50, 2032–2039 (2007). https://doi.org/10.1007/s10350-007-9062-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10350-007-9062-x