
Abstract
Purpose
Anorectal manometry is commonly used to investigate fecal incontinence. Traditional practice dictates that measurements are performed with the patient in the left-lateral position however, episodes of fecal incontinence usually occur in the erect position. The influence of erect posture on anorectal manometry has not been studied.
Methods
We examined the contribution of posture to commonly measured variables during manometry by performing assessment in the left-lateral position and the erect posture. Maximum mean resting pressure, vector volumes, and resting pressure gradient were compared.
Results
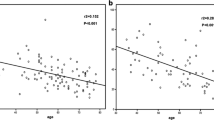
Complete data were available for 172 patients. Median age was 55 (interquartile range, 44–65) years. Thirty-seven (22 percent) patients were continent, and 135 (78 percent) were incontinent. Both resting pressure and vector volume increased significantly in the erect position for both continent (P = 0.008 and 0.001, respectively) and incontinent (P = 0.001 for both) patients. A significant negative correlation was seen between severity of incontinence and resting pressure in the erect posture and amount of change in maximum mean resting pressure from left-lateral to erect posture (Spearman coefficients = −0.203, −0.211, and P = 0.013, 0.017, respectively) but not with maximum mean resting pressure in the left-lateral position (Spearman coefficient = −0.119; P = 0.164).
Conclusions
Our study shows significant increase in measurements of manometric variables in the erect position. The increase may be related to anal cushions, which have a significant role in this position. The measurements in erect posture are better correlated with severity of incontinence and may be a more physiologic method of performing anorectal manometry.





Similar content being viewed by others


References
Whitehead WE, Wald A, Norton NJ. Priorities for treatment research from different professional perspectives. Gastroenterology 2004;126:S180–5.
Harris LD, Pope CE. “Squeeze” vs. resistance: an evaluation of the mechanism of sphincter competence. Clin Invest 1964;12:2272–8.
Katz LA, Kaufmann HJ, Spiro HM. Anal sphincter pressure characteristics. Gastroenterology 1967;52:513–8.
Collins CD, Duthie HL, Shelley T, Whittaker GE. Force in the anal canal and anal continence. Gut 1967;8:354–60.
Hancock BD. Measurement of anal pressure and motility. Gut 1976;17:645–51.
Bennet RC, Duthie HL. The functional importance of the internal anal sphincter. Br J Surg 1964;51:355–7.
Gibbons CP, Bannister JJ, Read NW. Role of constipation and anal hypertonia in the pathogenesis of haemorrhoids. Br J Surg 1988;75:656–60.
Pedersen IK, Christiansen J. A study of the physiological variation in anal manometry. Br J Surg 1988;76:67–71.
Yoshioka K, Keighley MR. The position of the patient does not adversely influence the results of the most clinically important measurements of anorectal function. Int J Colorectal Dis 1995;10:47–8.
Altomare DF, Rinaldi M, Veglia A, Guglielmi A, Sallustio PL, Tripoli G. Contribution of posture to the maintenance of anal continence. Int J Colorectal Dis 2001;16:51–4.
Jorge JM, Wexner SD. Etiology and management of fecal incontinence. Dis Colon Rectum 1993;36:77–97.
Rogers J, Levy DM, Henry MM, Misiewicz JJ. Pelvic floor neuropathy: a comparative study of diabetes mellitus and idiopathic faecal incontinence. Gut 1988;29:756–61.
Kielmann J, Bonnesen T. Anal profilometry: a method of investigation of the physiology of the anal canal and the pelvic floor. Dan Med Bull 1985;35:61–3.
Stojkovic SG, Balfour L, Burke D, Finan PJ, Sagar PM. Role of resting pressure gradient in the investigation of idiopathic faecal incontinence. Dis Colon Rectum 2002;45:668–73.
Felt-Bersma RJ, Klinkenberg-Knol EC, Meuwissen SG. Anorectal function investigations in incontinent and continent patients-differences and discriminatory value. Dis Colon Rectum 1990;33:479–86.
Sun WM, Read NW, Shorthouse AJ. Hypertensive anal cushions as a cause of the high anal canal pressures in patients with haemorrhoids. Br J Surg 1990;77:458–62.
Osterberg A, Graf W, Pahlman L. The longitudinal high-pressure zone profile in patients with faecal incontinence. Am J Surg 1999;159:112–7.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Thekkinkattil, D.K., Lim, M.K., Nicholls, M.J. et al. Contribution of Posture to Anorectal Manometric Measurements: Are the Measurements in Left-Lateral Position Physiologic?. Dis Colon Rectum 50, 2112–2119 (2007). https://doi.org/10.1007/s10350-007-9043-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10350-007-9043-0