
Abstract
Objective
The aim of this study was to investigate the clinicopathologic characteristics, diagnosis and differential diagnosis, molecular genetics, treatment and prognosis of solitary fibrous tumor (SFT).
Methods
The clinicopathological manifestations were analyzed retrospectively in 22 patients with surgically confirmed SFT.
Results
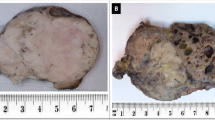
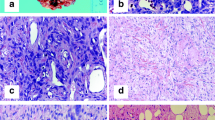
There were 12 male patients and 10 female patients, with the age range 33–67 (mean 48.62) years. The SFTs originated from different from parts of the body, including 13 in the chest, 2 in the lungs, 3 in the abdomen, 1 in the lumbosacral area, 2 in the pelvis, and 1 in the left shoulder. There were 19 benign and 3 malignant tumors. Major clinical presentations were local masses and compression symptoms. Microscopy: the tumor was composed of areas of alternating hypercellularity and hypocellularity. The tumor cells were spindle to short-spindle shaped and arranged in fascicular or storiform pattern and hemangiopericytoma-like structure was presented. Immunohistochemically, Vimentin positive rate was 100% (22/22), Bcl-2 positive rate was 95.5% (21/22), CD99 positive rate was 86.4% (19/22), CD34 positive rate was 81.8 (18/22), focally positive for P53, as well as negative CK, S100 and Desmin. Ki67 labelling index was 2%–30%.
Conclusion
SFT is a rare tumor which may be found in various parts of human body. SFT mostly is a benign tumor, but a few could be malignant. Its diagnosis mainly rely on its morphologic features and immunohistochemical profiles. The major treatment is to completely resect it by operation and long-term clinical follow-up is necessary.
Similar content being viewed by others

References
Perez-Ordonez B, Koutlas IG, Strich E, et al. Solitary fibrous tumor of the oral cavity: an uncommon location of a ubiquitous neoplasm. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 1999, 87: 589–593.
Torabi A, Lele SM, DiMaio D, et al. Lack of a common or characteristic cytogenetic anomaly in solitary fibrous tumor. Cancer Genet Cytogenet, 2008, 181: 60–64.
Gengler C, Guillou L. Solitary fibrous tumour and haemangiopericytoma: evolution of a concept. Histopathology, 2006, 48: 63–74.
Vallat-Decouvelaere AV, Dry SM, Fletcher CD. Atypical and malignant solitary fibrous tumours in extrathoracic locations: evidence of their comparability to intra-thoracic tumours. Am J Surg Pathol, 1998, 22: 1501–1511.
Hasegawa T, Matsuno Y, Shimoda T, et al. Extrathoracic solitary fibrous tumors: their histological variability and potentially aggressive behavior. Hum Pathol, 1999, 30: 1464–1473.
Gold JS, Antonescu CR, Hajdu C, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer, 2002, 94: 1057–1068.
Rossi G, Schirosi L, Giovanardi F, et al. Pleural malignant solitary fibrous tumor with sarcomatous overgrowth showing PDGFR beta mutation. Chest, 2006, 130: 581–583.
Ferreira EJ, Diaz JA. Solitary fibrous tumour of the pleura. Rev Chilena Cirugía, 2008, 60: 465–472.
Suster S, Fisher C, Moran CA. Expression of bcl-2 onooprotein in benign and malignant spindle cell tumors of soft tissue, skn serosal surfaces, and gastrointestinal tract. Am J Surg Pathol, 1998, 22: 863–872.
Kanthan R, Torkian B. Recurrent solitary fibrous tumor of the pleura with malignant transformation. Arch Pathol Lab Med, 2004, 128: 460–462.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhang, X., Wang, H., Wang, S. et al. Clinicopathological analysis of solitary fibrous tumor. Chin. -Ger. J. Clin. Oncol. 11, 282–284 (2012). https://doi.org/10.1007/s10330-011-0919-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10330-011-0919-z