
Abstract
Objective
The aim of our study was to explore the eikonic characteristic of skeletal metastasis of primary pulmonary carcinoma
Methods
Whole-body bone scans with 99Tcm methylene diphosphonate were performed in 258 patients with pathologically proven pulmonary carcinoma. The rate of skeletal metastasis, distribution of the metastatic lesions and their characteristics were analyzed.
Results
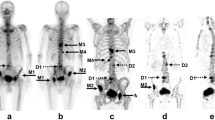
Among the total 258 patients, 142 cases developed skeletal metastasis. The overall rate of skeletal metastasis was 55.0%. The metastases located in axial skeleton were 49.6%, appendicular skeleton 36.0%, trunk bones of the axial skeleton 48.4%, and appendicular girdle skeleton 31.4%. Ribs, thoracic vertebrae, ilium and lumbar vertebrae had a higher rate of skeletal metastasis, which were 38.4%, 24.0%, 21.7%, 20.2%, respectively. 1252 lesions were detected including 406 at the left side of the body, 387 lesions at the middle position and 459 at the right side of the body. There was no significant difference in terms of number of lesions between left side and right side (χ2 = 3.3, P = 0.072). 1224 skeletal metastatic foci (97.8%) were presented as strong radioactive, 26 (2.1%) as mixed lesions, and 2 (0.2%) as low radioactive. According to the shape of lesions, there were 810 punctate lesions (71.5%), 159 (14.0%) lump form, 108 (9.5%) strip form and 56 (4.9%) lamellar form. The accumulative skeletal metastasis rate was 28.7% for the patients with one to three lesions. The metastasis rate decreased gradually as the number of metastatic lesions increased.
Conclusion
Skeletal metastasis is very common in patients with pulmonary carcinoma. Most skeletal metastases are characterized by strong radioactive and earlier punctate form; they often occur in the trunk bones of axial skeleton or appendicular girdles. The distribution of earlier metastases has not obvious regularity, and advanced skeletal metastases are widely and randomly distributed in the body, which are characterized by often concurrently multiple and polymorphous lesions.
Similar content being viewed by others

References
Chen G, Wang T, Yang YF, et al. Application and characteristics of whole-body bone scanning in detecting bone metastases in lung cancer. Chin J Med Imaging Technol (Chinese), 2009, 25: 1093–1095.
Zhang LH, Xie WH, Yu ZC. Clinical assessment of bone scanning in 1500 patients with lung cancer. Chin J Nucl Med (Chinese), 1999, 19: 6–7.
Yu T, Yin YF, Zhang XQ. Characteristics and the regular distribution of radionuclide bone scan on pulmonary carcinoma patients with osseous metastasis. J Chin Clin Med Imaging (Chinese), 2002, 13: 426–428.
Wang CY. Evaluation of bone metastasis characteristic of prostate cancer with 99mTc-MDP bone imaging. Pract J Cancer (Chinese), 2006, 21: 405–408.
Tang ZY. Contemporary oncology. Shanghai: Shanghai Medical University Press, 2000. 859–897.
Sugiura H, Yamada K, Sugiura T, et al. Predictors of survival in patients with bone metastasis of lung cancer. Clin Orthop Relat Res, 2008, 466: 729–736.
He J, Zeng ZC, Bi AH, et al. Clinical features and prognostic factors for the patients with bone metastases from non-small-cell lung cancer. Clin Med J China (Chinese), 2008, 15: 778–780.
Wilson MA, Calhoun FW. The distribution of skeletal metastases in breast and pulmonary cancer: Concise communication. J Nucl Med, 1981, 22: 594–597.
Otsuka S, Hanibuchi M, Ikuta K, et al. A bone metastasis model with osteolytic and osteoblastic properties of human lung cancer ACC-LC-319/bone2 in natural killer cell-depleted severe combined immunodeficient mice. Oncol Res, 2009, 17: 581–591.
Yin JJ, Pollock CB, Kelly K. Mechanisms of cancer metastasis to the bone. Cell Res, 2005, 15: 57–62.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, C., Zhang, X. Evaluation of eikonic characteristic of skeletal metastasis of primary pulmonary carcinoma with 99Tcm methylene diphosphonate whole-body bone scans. Chin. -Ger. J. Clin. Oncol. 9, 435–440 (2010). https://doi.org/10.1007/s10330-010-0655-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10330-010-0655-9