
Abstract
Background
A significant proportion of patients with connective tissue disease (CTD) have gastric esophageal reflux disease (GERD) symptoms despite receiving proton pump inhibitors (PPIs). Although pre-meal administration of PPIs is recommended in Western countries, the benefit of this administration timing in Japanese CTD patients with refractory GERD symptoms has not been proven.
Objective
To determine whether pre-dinner administration of PPIs is more efficacious for refractory GERD symptoms in Japanese CTD patients.
Methods
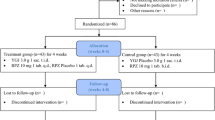
CTD patients receiving oral PPIs were instructed to take PPIs 1 h before dinner. Gastrointestinal symptoms were evaluated with frequency scale for the symptoms of GERD (FSSG) and gastrointestinal symptom rating scale (GSRS) before and after the intervention.
Results
Pre-dinner administration of PPIs significantly improved FSSG total score, from a median of 8 to 6.5 (P = 0.005). Pre-dinner administration was more effective in patients with overt GERD symptoms (from median 18 to 10, P < 0.001) than in those with mild GERD symptoms (from median 2 to 2, P = 0.201). In addition to reflux syndrome, pre-dinner administration of PPIs significantly decreased abdominal pain syndrome and constipation syndrome of GSRS.
Conclusion
Pre-dinner administration of PPIs may increase their efficacy in Japanese CTD patients with GERD, especially those with overt symptoms.



Similar content being viewed by others


References
Ling TC, Johnston BT. Esophageal investigations in connective tissue disease which tests are most appropriate? J Clin Gastroenterol. 2001;32:33–6.
Patti MG, Gasper WJ, Fisichella PM, Nipomnick I, Palazzo F. Gastroesophageal reflux disease and connective tissue disorders: pathophysiology and implications for treatment. J Gastrointest Surg. 2008;12:1900–6.
Daruwala C, Mercogliano G, Harder TP. Gastrointestinal manifestations of systemic lupus erythematosus and scleroderma. Clin Med Insights Gastroenterol. 2009;2:7–12.
Chong VH, Wang CL. Higher prevalence of gastrointestinal symptoms among patients with rheumatic disorders. Singapore Med J. 2008;48:419–24.
Ebert EC. The gastrointestinal complications of myositis. Aliment Pharmacol Ther. 2010;31:359–65.
Domsic R, Fasanella K, Bielefeldt K. Gastrointestinal manifestations of systemic sclerosis. Dig Dis Sci. 2008;53:1163–74.
Volter F, Fain O, Mathieu E, Thomas M. Esophageal function and Sjögren’s syndrome. Dig Dis Sci. 2004;49:248–53.
Marshall JB, Kretschmar JM, Gerhardt DC, Winship DH, Winn D, Treadwell EL, et al. Gastrointestinal manifestations of mixed connective tissue disease. Gastroenterology. 1990;98:1232–8.
Fujiwara Y, Arakawa T. Epidemiology and clinical characteristics of GERD in the Japanese population. J Gastroenterol. 2009;44:518–34.
Hatlebakk JG, Katz PO, Camacho-Lobato L, Catell DO. Proton pump inhibitors: better acid suppression when taken before a meal than without a meal. Aliment Pharmacol Ther. 2000;14:1267–72.
Morise K, Iizuka A, Inagaki T, Sugie M, Matsunaga Y, Nakata K, et al. Clinical effect of omeprazole, a gastric proton pump inhibitor—comparative study on morning dose and bed-time dose in the treatment of peptic ulcer. Yakuri to Rinsyo. 1988;16:593–608.
Shinomura K, Kaneyama S, Miyazaki Y, Okuda S, Iiishi H, Himeno S, et al. Mod Phys. 1994;14:69–84.
Tateno M, Nakamura M. Phase I study of lansoprazole (AG-1749) antiulcer agent—capsule form—. Rinsyo Iyaku. 1991;7:51–62.
Yasuda S, Ohnishi A, Ogawa T, Tomono Y, Hasegawa J, Nakai H, et al. Pharmacokinetic properties of E3810, a new proton pump inhibitor, in healthy male volunteers. Int J Clin Pharmacol Ther. 1994;32:466–73.
Kusano M, Shimoyama Y, Sugimoto S, Kawamura O, Maeda M, Minashi K, et al. Development and evaluation of FSSG: frequency scale for the symptoms of GERD. J Gastroenterol. 2004;39:888–91.
Dimenas E, Glise H, Hallerback B, Hernqvist H, Svedlund J, Wiklund I. Well-being and gastrointestinal symptoms among patients referred to endoscopy owing to suspected duodenal ulcer. Scand J Gastroenterol. 1995;30:1046–52.
Kinoshita Y, Ishihara S. Causes of, and therapeutic approaches for, proton pump inhibitor-resistant gastroesophageal reflux disease in Asia. Therap Adv Gastroenterol. 2008;1:191–9.
Fass R, Sifrim D. Management of heartburn not responding to proton pump inhibitors. Gut. 2009;58:295–309.
Miki M, Adachi K, Azumi T, Koshino K, Furuta K, Kinoshita Y. A comparative study of intragastric acidity during post-breakfast and pre-dinner administration of low-dose proton pump inhibitors: a randomized three-way cross over study. Aliment Pharmacol Ther. 2006;24:1445–51.
Xie HG, Stein CM, Kim RB, Wilikinson GR, Flockhart DA, Wood AJ. Allelic, genotypic and phenotypic distributions of S-mephenytoin 4′-hydroxylase (CYP2C19) in healthy Caucasian populations of European descent throughout the world. Pharmacogenetics. 1999;9:539–49.
Furuta T, Shirai N, Kodaira M, Sugimoto M, Nogaki A, Kuriyama S, et al. Pharmacogenomics-based tailored versus standard therapeutic regimen for eradication of H. pylori. Clin Pharmacol Ther. 2007;81:521–8.
Acknowledgments
We thank Dr. H. Iwata (Department of Surgery, Shinkatsushika Hospital, Tokyo), a board-certified gastroenterologist, for evaluation of endoscopic findings and valuable discussion. This work was supported in part by Grants-in-Aids for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology, the Japanese Government and by Global COE Program (Global Center for Education and Research in Immune System Regulation and Treatment), MEXT, Japan.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article
Cite this article
Iwata, A., Ikeda, K., Hirose, K. et al. Pre-dinner administration increases the efficacy of proton pump inhibitors on refractory GERD symptoms in connective tissue disease patients. Mod Rheumatol 23, 357–364 (2013). https://doi.org/10.1007/s10165-012-0662-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10165-012-0662-5