
Abstract
Background
Although more than 40 years have passed since IgA nephropathy (IgAN) was first reported, predicting the renal outcome of individual IgAN patients remains difficult. Emerging epidemiologic evidence indicates that overweight and obesity are risk factors for end-stage renal disease. We aimed to elucidate the outcome of overweight IgAN patients and improve our ability to predict the progression of IgAN based on a combination of body mass index (BMI) and histopathological parameters, including maximal glomerular area (Max GA).
Methods
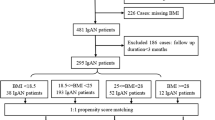
Forty-three adult IgAN patients whose estimated glomerular filtration rate was ≥50 ml/min/1.73 m2 were enrolled in this study. Renal biopsy specimens were evaluated according to the Oxford classification of IgAN. A Kaplan–Meier analysis and the multivariate Cox proportional hazards method were used to evaluate 10-year kidney survival and the impact of covariates. The ability of factors to predict the progression of IgAN was evaluated by their diagnostic odds ratio (DOR).
Results
A BMI ≥25 kg/m2 was found to be an independent predictor of a ≥1.5-fold increase in serum creatinine value (DOR 7.4). The combination of BMI ≥25 kg/m2, Max GA ≥42,900 μm2, and presence of mesangial hypercellularity (Oxford M1) optimally raised predictive power for disease progression of IgAN (DOR 26.0).
Conclusion
A combination of BMI ≥25 kg/m2, the Oxford classification M1, and a Max GA ≥42,900 μm2 can serve as a predictor of long-term renal outcome of IgAN.




Similar content being viewed by others
References
Nenov VD, Taal MW, Sakharova OV, Brenner BM. Multi-hit nature of chronic renal disease. Curr Opin Nephrol Hypertens. 2000;9:85–97.
Taal MW, Brenner BM. Predicting initiation and progression of chronic kidney disease: developing renal risk scores. Kidney Int. 2006;70:1694–705.
Barratt J, Feehally J. IgA nephropathy. J Am Soc Nephrol. 2005;16:2088–97.
Berthoux FC, Mohey H, Afiani A. Natural history of primary IgA nephropathy. Semin Nephrol. 2008;28:4–9.
Donadio JV, Bergstralh EJ, Grande JP, Rademcher DM. Proteinuria patterns and their association with subsequent end-stage renal disease in IgA nephropathy. Nephrol Dial Transplant. 2002;17:1197–203.
Goto M, Kawamura T, Wakai K, Ando M, Endoh M, Tomino Y. Risk stratification for progression of IgA nephropathy using a decision tree induction algorithm. Nephrol Dial Transplant. 2009;24:1242–7.
Glassock RJ. IgA nephropathy: challenges and opportunities. Cleve Clin J Med. 2008;75:569–76.
Roufosse CA, Cook HT. Pathological predictors of prognosis in immunoglobulin A nephropathy: a review. Curr Opin Nephrol Hypertens. 2009;18:212–9.
Wang Y, Chen X, Song Y, Caballero B, Cheskin LJ. Association between obesity and kidney disease: a systematic review and meta-analysis. Kidney Int. 2008;73:19–33.
Liu H, Shi H, Yu J, Chen F, Jiang Q, Hu D. Obesity and chronic kidney disease in patients with chronic heart failure: an insight from the China Heart Survey. Clin Exp Nephrol. 2011;15:522–8.
Hsu CY, McCulloch CE, Iribarren C, Darbinian J, Go AS. Body mass index and risk for end-stage renal disease. Ann Intern Med. 2006;144:21–8.
Zoccali C. The obesity epidemics in ESRD: from wasting to waist? Nephrol Dial Tranplant. 2009;24:376–80.
Iseki K, Ikemiya Y, Kinjo K, Inoue T, Iseki C, Takishita S. Body mass index and the risk of development of end-stage renal disease in a screened cohort. Kidney Int. 2004;65:1870–6.
Kato S, Nazneen A, Nakashima Y, Razzaque MS, Nishino T, Furusu A, et al. Pathological influence of obesity on renal structural changes in chronic kidney disease. Clin Exp Nephrol. 2009;13:332–40.
Afshinnia F, Wilt TJ, Duval S, Esmaeili A, Ibrahim HN. Weight loss and proteinuria: systematic review of clinical trials and comparative cohorts. Nephrol Dial Transplant. 2010;25:1173–83.
Kataoka H, Ohara M, Honda K, Mochizuki T, Nitta K. Maximal glomerular diameter as a 10-year prognostic indicator for IgA nephropathy. Nephrol Dial Transplant. 2011;26:3937–43.
Roberts IS, Cook HT, Troyanov S, Alpers CE, Amore A, Barratt J, et al. The Oxford classification of IgA nephropathy: pathology definitions, correlations, and reproducibility. Kidney Int. 2009;76:546–56.
Imai E, Horio M, Nitta K, Yamagata K, Iseki K, Tsukamoto Y, et al. Modification of the Modification of Diet in Renal Disease (MDRD) Study equation for Japan. Am J Kidney Dis. 2007;50:927–37.
Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006;295:1549–55.
Radford MG Jr, Donadio JV Jr, Bergstralh EJ, Grande JP. Predicting renal outcome in IgA nephropathy. J Am Soc Nephrol. 1997;8:199–207.
Suzuki K, Honda K, Tanabe K, Toma H, Nihei H, Yamaguchi Y. Incidence of latent mesangial IgA deposition in renal allograft donors in Japan. Kidney Int. 2003;63:2286–94.
Glas AS, Lijmer JG, Prins MH, Bonsel GJ, Bossuyt PM. The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol. 2003;56:1129–35.
Blüher M. The distinction of metabolically ‘healthy’ from ‘unhealthy’ obese individuals. Curr Opin Lipidol. 2010;21:38–43.
Wu Y, Liu Z, Xiang Z, Zeng C, Chen Z, Ma X, et al. Obesity-related glomerulopathy: insights from gene expression profiles of the glomeruli derived from renal biopsy samples. Endocrinology. 2006;147:44–50.
Navaneethan SD, Yehnert H, Moustarah F, Schreiber MJ, Schauer PR, Beddhu S. Weight loss interventions in chronic kidney disease: a systematic review and meta-analysis. Clin J Am Soc Nephrol. 2009;4:1565–74.
Schrijvers BF, Rasch R, Tilton RG, Flyvbjerg A. High protein-induced glomerular hypertrophy is vascular endothelial growth factor-dependent. Kidney Int. 2002;61:1600–4.
Yoshida Y, Kawamura T, Ikoma M, Fogo A, Ichikawa I. Effects of antihypertensive drugs on glomerular morphology. Kidney Int. 1989;36:626–35.
Xu ZG, Yoo TH, Ryu DR, Cheon Park H, Ha SK, Han DS, et al. Angiotensin II receptor blocker inhibits p27Kip1 expression in glucose-stimulated podocytes and in diabetic glomeruli. Kidney Int. 2005;67:944–52.
Guo C, Martinez-Vasquez D, Mendez GP, Toniolo MF, Tao TM, Oestreicher EM, et al. Mineralocorticoid receptor antagonist reduces renal injury in rodent models of types 1 and 2 diabetes mellitus. Endocrinology. 2006;147:5363–73.
Acknowledgments
We would like to express our appreciation for providing us with statistical advice to Sadao Ishimura, Ph.D., D.Sc., Laboratory of Mathematics, Tsurumi University School of Dental Medicine, Yokohama, Japan.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Terms used to evaluate a diagnostic test:
Sensitivity (Se): The proportion of positive test results among those with the target disease.
Specificity (Sp): The proportion of negative test results among those without the disease.
Positive predictive value (PPV): Probability of a disease being present in a patient with a positive test result.
Negative predictive value (NPV): Probability of a patient with a negative test result not having a disease.
Positive likelihood ratio (+LR): The ratio of evaluating how much more frequent a positive test is found in diseased versus non-diseased individuals.
Diagnostic odds ratio (DOR): A global measure of test performance calculated by using the formula: [Se/(1 − Sp)]/[(1 − Se)/Sp].
About this article
Cite this article
Kataoka, H., Ohara, M., Shibui, K. et al. Overweight and obesity accelerate the progression of IgA nephropathy: prognostic utility of a combination of BMI and histopathological parameters. Clin Exp Nephrol 16, 706–712 (2012). https://doi.org/10.1007/s10157-012-0613-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-012-0613-7