
Abstract
Background
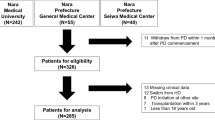
In Japan, the population of patients on peritoneal dialysis (PD) is <4% of the total number of patients with end-stage renal disease. Few systemic analyses have examined why the number of PD patients has not increased in Japan. We organized a registry to analyze PD patients and retrospectively investigated 561 PD patients (about 5% of all Japanese PD patients) from 13 hospitals in the Tokai area for 3 years from 2005.
Methods
We investigated background, physical status, laboratory data, status of PD therapy, and the occurrence of PD-related complications, and analyzed reasons for withdrawal from PD.
Results
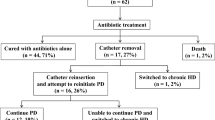
Nutrition did not change significantly during our observation. Urinary volume showed continued decreases after the introduction period. In contrast, PD fluid demand and ultrafiltration volume were significantly increased. For calcium metabolism, multiple phosphate binders were required after the second year of PD therapy. Early drop-out within 3 years after starting PD therapy comprised 50.9% of total withdrawals, with PD-related peritonitis as the most common reason, mainly caused by Gram-positive organisms. Incidence of peritonitis was 42.8 months/patient. Culture-negative results were obtained for 32% of peritonitis cultures. Diabetes affects the prognosis of PD therapy, but not the incidence of peritonitis.
Conclusion
We examined clinical status over 3 years in the Tokai area. The results suggest that the incidence of peritonitis needs to be decreased to prevent early withdrawal of PD patients. Education systems to decrease the incidence of peritonitis and techniques to decrease culture-negative results might be important for improving the prognosis of peritonitis.





Similar content being viewed by others

References
Japanese Society for Dialysis Therapy Committee of Renal Data Registry. An overview of regular dialysis treatment in Japan as of Dec 31, 2009; JSDT website: http://www.jsdt.or.jp/.
Cueto-Manzano AM, Rojas-Campos E. Status of renal replacement therapy and peritoneal dialysis in Mexico. Perit Dial Int. 2007;27:142–8.
Yu AW, Chau KF, Ho YW, Li PK. Development of the “peritoneal dialysis first” model in Hong Kong. Perit Dial Int. 2007;27:S53–5.
Kawaguchi Y, Ishizaki T, Imada A, Oohira S, Kuriyama S, Nakamoto H, et al. Searching for the reasons for drop-out from peritoneal dialysis: a nationwide survey in Japan. Perit Dial Int. 2003;23:S175–7.
Kawaguchi Y. Various obstacles to peritoneal dialysis development in Japan: too much money? Too much fear? Perit Dial Int. 2007;27:S56–8.
Nakamoto H, Kawaguchi Y, Suzuki H. Is technique survival on peritoneal dialysis better in Japan? Perit Dial Int. 2006;26:136–43.
Masakane I, Tsubakihara Y, Akiba T, Watanabe Y, Iseki K. The most recent trends of peritoneal dialysis in Japan. Perit Dial Int. 2008;28:S27–31.
Moncrief JW, Popovich RP, Broadrick LJ, He ZZ, Simmons EE, Tate RA. The Moncrief-Popovich catheter. A new peritoneal access technique for patients on peritoneal dialysis. ASAIO J. 1993;39:62–5.
Piraino B, Bailie GR, Bernardini J, Boeschoten E, Gupta A, Holmes C, et al. Peritoneal dialysis-related infections recommendations: 2005 update. Perit Dial Int. 2005;25:107–31.
Li PK, Szeto CC, Piraino B, Bernardini J, Figueiredo AE, Gupta A, et al. ISPD guidelines/recommendation. Peritoneal dialysis-related infections recommendations: 2010 update. Perit Dial Int. 2010;30:393–423.
Okada S, Inoue T, Nakamoto H, Ikeda N, Sugahara S, Shoda J, et al. Residual renal function plays an important role in regulating parathyroid hormone in patients on continuous ambulatory peritoneal dialysis. Adv Perit Dial. 2007;23:150–4.
Kawanishi H, Kawaguchi Y, Fukui H, Hara S, Imada A, Kubo H, et al. Encapsulating peritoneal sclerosis in Japan: a prospective, controlled, multicenter study. Am J Kidney Dis. 2004;44:729–37.
Chung SH, Heimbürger O, Lindholm B, Lee HB. Peritoneal dialysis patient survival: a comparison between a Swedish and a Korean centre. Nephrol Dial Transplant. 2005;20:1207–13.
Mactier R. Peritonitis is still the achilles’ heel of peritoneal dialysis. Perit Dial Int. 2009;29:262–6.
Abraham G, Pratap B, Sankarasubbaiyan S, Govindan P, Nayak KS, Sheriff R, et al. Chronic peritoneal dialysis in South Asia—challenges and future. Perit Dial Int. 2008;28:13–9.
Davenport A. Peritonitis remains the major clinical complication of peritoneal dialysis: the London, UK, peritonitis audit 2002–2003. Perit Dial Int. 2009;29:297–302.
Bernardini J, Price V, Figueiredo A, Riemann A, Leung D. International survey of peritoneal dialysis training program. Perit Dial Int. 2006;26:658–63.
Huisman RM, Nieuwenhuizen MG, Th de Charro F. Patient-related and centre-related factors influencing technique survival of peritoneal dialysis in The Netherlands. Nephrol Dial Transplant. 2002;17:1655–60.
Plantinga LC, Fink NE, Finkelstein FO, Powe NR, Jaar BG. Association of peritoneal dialysis clinic size with clinical outcomes. Perit Dial Int. 2009;29:285–91.
Han SH, Lee SC, Ahn SV, Lee JE, Choi HY, Kim BS, et al. Improving outcome of CAPD: twenty-five years’ experience in a single Korean center. Perit Dial Int. 2007;27:432–40.
Russo R, Manili L, Tiraboschi G, Amar K, De Luca M, Alberghini E, et al. Patient re-training in peritoneal dialysis: why and when it is needed. Kidney Int. 2006;103:S127–32.
Chow KM, Szeto CC, Leung CB, Law MC, Kawan BC, Li PK. Adherence to peritoneal dialysis training schedule. Nephrol Dial Transplant. 2007;22:545–51.
Kuriyama S. Peritoneal dialysis in patients with diabetes: are the benefits greater than the disadvantages? Perit Dial Int. 2007;27:S190–5.
Paniagua R, Orihuela O, Ventura MD, Avila-Díaz M, Cisneros A, Vicenté-Martínez M, et al. Echocardiographic, electrocardiographic and blood pressure changes induced by icodextrin solution in diabetic patients on peritoneal dialysis. Kidney Int. 2008;108:S125–30.
Ramo’n P, Ventura M, A’vila-Díaz M, Cisneros A, Vicenté-Martínez M, Furlong M, et al. Icodextrin improves metabolic and fluid management in high and high-average transport diabetic patients. Perit Dial Int. 2009;29:422–32.
Lin A, Qian J, Li X, Yu X, Liu W, Sun Y, et al. Randomized controlled trial of icodextrin versus glucose containing peritoneal dialysis fluid. Clin J Am Soc Nephrol. 2009;4:1799–804.
Martinez-Mier G, Garcia-Almazan E, Reyes-Devesa HE, Garcia-Garcia V, Cano-Gutierrez S, Mora y Fermin R, et al. Abdominal wall hernia in end-stage renal disease patients on peritoneal dialysis. Perit Dial Int. 2008;28:391–6.
Twardowski ZJ. PET—a simpler approach for determining prescriptions for adequate dialysis therapy. Adv Perit Dial. 1990;6:186–91.
Acknowledgments
The authors wish to offer special thanks to Ms. Onishi and Ms. Kato for their assistance in creating the database, and to Mr. Nakamura for help with statistical analyses. We are also grateful to the medical and co-medical staff who helped with registration of PD patients and data collection for our registration system.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Mizuno, M., Ito, Y., Tanaka, A. et al. Peritonitis is still an important factor for withdrawal from peritoneal dialysis therapy in the Tokai area of Japan. Clin Exp Nephrol 15, 727–737 (2011). https://doi.org/10.1007/s10157-011-0471-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-011-0471-8