
Abstract
Background
Fistula-in-ano has a reported incidence of 31–34%. Besides fistulotomy, options for fistula repair are seton placement, endorectal advancement flap (ERAF), fibrin sealant, anal fistula plug and ligation of the intersphincteric fistula tract. Despite having a reported success rate as high as 75–98%, ERAF is not without complications, including flap breakdown, recurrence and fecal incontinence. Traditionally, maintaining a broad base to preserve blood supply has been advocated to reduce flap failure. And the aim of the present study was to evaluate outcomes of adult patients who underwent ERAF for complex fistula-in-ano with the use of intraoperative fluorescence angiography (FA) at our institution between July 2014 and July 2016.
Methods
We retrospectively reviewed consecutive cases of complex fistula-in-ano repair with ERAF and FA from a prospectively maintained dataset of adult patients with complex fistula-in-ano. Demographics, intraoperative data and 60-day outcomes were recorded and reviewed.
Results
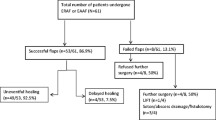
Six patients [five males and one female with a mean age of 40 years (range 25–46 years)], with a total of seven fistulas, were identified. Six (85.7%) of these patients had undergone prior surgery for fistula-in-ano. No recurrences or complications of any type were noted at 2-week and 8-week follow-up. The majority of patients (71.4%) required flap revision based on intraoperative FA prior to flap fixation.
Conclusions
FA is safe and offers real-time assessment of flap perfusion prior to and after fixation in anal fistula repair. The rate of flap ischemia may be underestimated, and therefore, to improve outcomes in ERAF, intraoperative FA should be included in the surgical armamentarium.


Similar content being viewed by others


References
Lohsiriwat V, Yodying H, Lohsiriwat D (2010) Incidence and factors influencing the development of fistula-in-ano after incision and drainage of perianal abscesses. J Med Assoc Thail 93(1):61–65
Ramanujam PS, Prasad ML, Abcarian H, Tan AB (1984) Perianal abscesses and fistulas. A study of 1023 patients. 2. Dis Colon Rectum 27(9):593–597
Farmer RG, Hawk WA, Turnbull RB Jr (1975) Clinical patterns in Crohn’s disease: a statistical study of 615 cases. Gastroenterology 68(4 Pt 1):627–635
Visscher AP, Schuur D, Roos R et al (2015) Long-term follow-up after surgery for simple and complex cryptoglandular fistulas: fecal incontinence and impact on quality of life. Dis Colon Rectum 58(5):533–539
Hämäläinen KP, Sainio AP (1997) Cutting seton for anal fistulas: high risk of minor control defects. Dis Colon Rectum 40(12):1443–1446
Blumetti J, Abcarian A, Quinteros F et al (2012) Evolution of treatment of fistula-in-ano. World J Surg 36(5):1162–1167
Göttgens KW, Smeets RR, Stassen LP et al (2015) Systematic review and meta-analysis of surgical interventions for high cryptoglandular perianal fistula. Int J Colorectal Dis 30(5):583–593
Sheikh P, Baakza A (2014) Management of fistula-in-ano—the current evidence. Indian J Surg 76(6):482–486
Dudukgian H, Abcarian H (2011) Why do we have so much trouble treating anal fistula? World J Gastroenterol 17(28):3292–3296
Ommer A, Wenger FA, Rolfs T et al (2008) Continence disorders after anal surgery–a relevant problem? Int J Colorectal Dis 23(11):1023–1031
Golub RW, Wise WE Jr, Kerner BA et al (1997) Endorectal mucosal advancement flap: the preferred method for complex cryptoglandular fistula-in-ano. J Gastrointest Surg 1(5):487–491
Soltani A, Kaiser AM (2010) Endorectal advancement flap for cryptoglandular or Crohn’s fistula-in-ano. Dis Colon Rectum 53(4):486–495
Sonoda T, Hull T, Piedmonte MR et al (2002) Outcomes of primary repair of anorectal and rectovaginal fistulas using the endorectal advancement flap. Dis Colon Rectum 45(12):1622–1628
Jarrar A, Church J (2011) Advancement flap repair: a good option for complex anorectal fistulas. Dis Colon Rectum 54(12):1537–1541
Fisher OM, Raptis DA, Vetter D et al (2015) An outcome and cost analysis of anal fistula plug insertion vs endorectal advancement flap for complex anal fistulae. Colorectal Dis 17(7):619–626
Tan KK, Alsuwaigh R, Tan AM et al (2012) To LIFT or to flap? Which surgery to perform following seton insertion for high anal fistula? Dis Colon Rectum 55(12):1273–1277
Stremitzer S, Riss S, Swoboda P et al (2012) Repeat endorectal advancement flap after flap breakdown and recurrence of fistula-in-ano–is it an option? Colorectal Dis 14(11):1389–1393
Mizrahi N, Wexner SD, Zmora O et al (2002) Endorectal advancement flap: are there predictors of failure? Dis Colon Rectum 45(12):1616–1621
Jones IT, Fazio VW, Jagelman DG (1987) The use of transanal rectal advancement flaps in the management of fistulas involving the anorectum. Dis Colon Rectum 30(12):919–923
Christoforidis D, Pieh MC, Madoff RD, Mellgren AF (2009) Treatment of transsphincteric anal fistulas by endorectal advancement flap or collagen fistula plug: a comparative study. Dis Colon Rectum 52:18–22
Alander JT, Kaartinen I, Laakso A et al (2012) A review of indocyanine green fluorescent imaging in surgery. Int J Biomed Imaging 2012:940585
Owens SL (1996) Indocyanine green angiography. Br J Ophthalmol 80(3):263–266
Jafari MD, Wexner SD, Martz JE et al (2015) Perfusion assessment in laparoscopic left sided/anterior resection (PILLAR II): a multi-institutional study. J Am Coll Surg 220:82–92
Atallah SB, Albert MR, de Beche-Adams TC et al (2013) Application of laser-assisted indocyanine green fluorescent angiography for the assessment of tissue perfusion of anodermal advancement flaps. Dis Colon Rectum 56:797
Turner J, Clark C (2016) Fluorescence imaging in anorectal advancement flaps. Dis Colon Rectum 59(7):700
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed is studies involving human participation were conducted in accordance with the standards of the institution and approved by the institution’s institutional review board.
Informed consent
As this is a study based on data from a databank, informed consent for patients enrolled is not applicable.
Rights and permissions
About this article

Cite this article
Turner, J.S., Okonkwo, A., Chase, A. et al. Early outcomes of fluorescence angiography in the setting of endorectal mucosa advancement flaps. Tech Coloproctol 22, 25–30 (2018). https://doi.org/10.1007/s10151-017-1732-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-017-1732-7