
Abstract
Background
The aim of this study was to determine whether mobilization of the splenic flexure during anterior resection is associated with an increased number of complications.
Methods
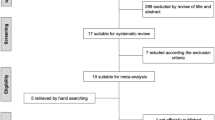
This is a retrospective cohort analysis of all non-emergent anterior resections with anastomosis (open and laparoscopic) between January 2005 and December 2009 from the American College of Surgeons National Surgical Quality Improvement Program. Infectious, renal, and pulmonary adverse events as well as operative times were analyzed for cases with splenic flexure mobilization as compared to no mobilization. We then constructed multivariate models to identify risk factors for postsurgical adverse events.
Results
During the 5-year study period, 6,324 (57 %) open resections and 4,788 (43 %) laparoscopic resections were performed. Mobilization of the splenic flexure was associated with an increase in operating room time (204 vs 172 min, p < 0.0001). Although anastomotic leaks were not recorded, there was no difference in organ space infections (3.9 vs 3.7 %, p = 0.7) or return to operating room events between the two groups. However, patients who underwent splenic flexure mobilization had significantly more superficial surgical site infections (10.6 vs 8.4 %, p < 0.0002). Multivariate analysis accounting for laparoscopic or open surgery and standard preoperative and intraoperative variables demonstrated a persistent increase in superficial surgical site infections for patients with splenic flexure mobilization.
Conclusions
Operating room times are longer and superficial surgical site infections are more common when the splenic flexure is mobilized. The absolute indications for splenic flexure mobilization should be addressed in further research.
Similar content being viewed by others


References
Ludwig KA, Kosinski L (2012) Is splenic flexure mobilization necessary in laparoscopic anterior resection? Another view. Dis Colon Rectum 55:1198
Chand M, Miskovic D, Parvaiz AC (2012) Is splenic flexure mobilization necessary in laparoscopic anterior resection? Dis Colon Rectum 55:1195
Cheung YM, Lange MM, Buunen M, Lange JF (2009) Current technique of laparoscopic total mesorectal excision (TME): an international questionnaire among 368 surgeons. Surg Endosc 23:2796
Marsden M, Conti J, Zeidan S et al (2012) The selective use of splenic flexure mobilization is safe in both laparoscopic and open anterior resections. Colorectal Dis 14:1255–1261
Park JS, Kang SB, Kim DW et al (2009) Laparoscopic versus open resection without splenic flexure mobilization for the treatment of rectum and sigmoid cancer: a study from a single institution that selectively used splenic flexure mobilization. Surg Laparosc Endosc Percutan Tech 19:62–68
Kim J, Choi DJ, Kim SH (2009) Laparoscopic rectal resection without splenic flexure mobilization: a prospective study assessing anastomotic safety. Hepatogastroenterology 56:1354–1358
American College of Surgeons National Surgical Quality Improvement Program (2011). http://www.acsnsqip.org, Chicago, IL, 2011. Accessed 27 July 2011
Health Information Privacy. http://www.hhs.gov/ocr/privacy, Washington, DC, 2011. Accessed 27 July 2011
Khuri SF, Daley J, Henderson W et al (1998) The Department of Veterans Affairs’ NSQIP: the first national, validated, outcome-based, risk-adjusted, and peer-controlled program for the measurement and enhancement of the quality of surgical care. National VA Surgical Quality Improvement Program. Ann Surg 228:491–507
American College of Surgeons National Surgical Quality Improvement Program: User Guide for the 2008 Participant Use Data File. https://www.acsnsqip.org/main/puf/documents/pdfs/ACS_NSQIP_Participant_User_Data_File_User_Guide.pdf, Chicago, IL, 2011. Accessed 27 July 2011
Ingraham AM, Cohen ME, Bilimoria KY et al (2010) Comparison of hospital performance in nonemergency versus emergency colorectal operations at 142 hospitals. J Am Coll Surg 2010:155–165
Brennan DJ, Moynagh M, Brannigan AE, Gleeson F, Rowland M, O’Connell PR (2007) Routine mobilization of the splenic flexure is not necessary during anterior resection for rectal cancer. Dis Colon Rectum 50:302–307
Thum-Umnuaysuk S, Boonyapibal A, Geng YY, Pattana-Arun J (2012) Lengthening of the colon for low rectal anastomosis in a cadaveric study: how much can we gain? Tech Coloproctol. doi:10.1007/s10151-012-0930-6
Akiyoshi T, Kuroyananagi H, Oya M et al (2010) Factors affecting difficulty of laparoscopic surgery for left-sided colon cancer. Surg Endosc 24:2749–2754
Hiranyakas A, Da Silva G, Denoya P, Shawki S, Wexner SD (2012) Colorectal anastomotic stricture: is it associated with inadequate colonic mobilization? Tech Coloproctol. doi:10.1007/s10151-012-0929-z
Gezen C, Altuntas YE, Kement M et al (2012) Complete versus partial mobilization of splenic flexure during laparoscopic low anterior resection for rectal tumors: a comparative study. J Laparoendosc Adv Surg Tech A 22:392–396
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the American College of Surgeons National Surgical Quality Improvement Program are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Rights and permissions
About this article
Cite this article
Carlson, R.M., Roberts, P.L., Hall, J.F. et al. What are 30-day postoperative outcomes following splenic flexure mobilization during anterior resection?. Tech Coloproctol 18, 257–264 (2014). https://doi.org/10.1007/s10151-013-1049-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-013-1049-0