
Abstract
Introduction
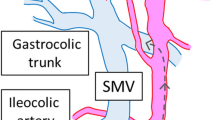
When performing a colonic resection for cancerous lesions, a complete mesocolic excision (CME) can lead to improved oncologic results. The CME along with the high vessel ligation, meaning the ligation of the supplying vessels close to their origin, can ensure maximal lymph node harvest. The principles of CME and high ligation have been applied by us during colonic resections for cancer. We present our experience with tumors of the proximal colon, for which a radical right hemicolectomy has been performed.
Patients and methods
Between 1989 and 2008, we performed a right hemicolectomy in 115 patients. The mean age was 65.6 years (range 35–86). The tumor was located in the cecum in 37% of patients, the ascending colon in 58% of the patients and the hepatic flexure in 5% of the patients. All patients underwent complete mesocolic excision and high ligation of the supplying vessels. A total of 93% (107/115) of these operations were performed on an elective basis. Out of all patients, 48 (42%) received adjuvant chemotherapy.
Results
No patient died during the immediate postoperative period. The postoperative morbidity was 13.9% (16/115). One patient developed a metachronous rectal carcinoma 28 months after his surgery, for which he underwent an abdoperineal resection. The 5-year survival rate lies at 72.4% (55/76). Twenty patients (26.3%) died due to metastatic disease before completing 5 years of follow-up. The remaining 39 patients have been operated after the end of 2004 and have therefore not completed 5 years from the day of their operation yet.
Conclusions
There is no doubt that standardized oncologic surgery shows particular importance by reducing the rate of local recurrence and achieving increased survival. It is important to remember that colon cancer treatment today is multimodal and that the improvement in patients’ survival in the last decades is surely linked with the improvement in chemotherapy and the advances in the agents used. However, optimal surgery is with no doubt an important element of good oncological outcome, as the experience with rectal cancer treatment has taught us.
Similar content being viewed by others


References
Heald RJ (1988) The ‘Holy Plane’ of rectal surgery. J R Soc Med 81:503–508
Chen SL, Bilchik AJ (2006) More extensive nodal dissection improves survival for stages I to III of colon cancer: a population-based study. Ann Surg 244:602–610
Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S (2009) Standardized surgery for colonic cancer: complete mesocolic excision and central ligation—technical notes and outcome. Colorectal Dis 11:354–365
Tornroos A, Garvin S, Olsson H (2009) The number of identified lymph node metastases increases continuously with increased total lymph node recovery in pT3 colon cancer. Acta Oncol 48:1152–1156
Mammen JM, James LE, Molloy M, Williams A, Wray CJ, Sussman JJ (2007) The relationship of lymph node dissection and colon cancer survival in the Veterans Affairs Central Cancer Registry. Am J Surg 194:349–354
Conflict of interest
The author declares that he has no conflict of interest related to the publication of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pramateftakis, M.G. Optimizing colonic cancer surgery: high ligation and complete mesocolic excision during right hemicolectomy. Tech Coloproctol 14 (Suppl 1), 49–51 (2010). https://doi.org/10.1007/s10151-010-0609-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-010-0609-9