
Abstract
Introduction
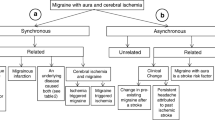
Migraine with aura (MA) is a frequent stroke simulator that can lead to erroneous diagnosis and subsequent unnecessary acute or secondary prevention treatments. We analyzed clinical and laboratory data of migraine with aura and ischemic stroke patients to detect differences that could help in the diagnosis.
Methods
Retrospective analysis of a consecutive register of code strokes between January 2005 and June 2020. Diagnosis of ischemic stroke or MA was collected. Multivariable logistic regression analyses were performed to test associations between clinical and blood data with ischemic stroke.
Results
Of 3140 code strokes, 2424 (77.2%) were ischemic strokes and 34 (1.1%) were MA. Migraine cases were younger, more frequently females and with lower prevalence of vascular risk factors. Initial NIHSS was lower in MA cases, but no differences were seen in fibrinolysis rate (30%). Blood test showed lower levels of glucose, D-dimer, and fibrinogen in MA cases. Multivariable model showed and independent association for ischemic stroke with age [OR, (95%CI): 1.09, (1.07–1.12, p < 0.001], male sex [OR, (95%CI): 4.47, (3.80–5.13), p < 0.001], initial NIHSS [OR, (95%CI): 1.21, (1.07–1.34), p < 0.01], and fibrinogen levels [OR, (95%CI): 1.01, (1.00–1.01), p < 0.05]. A model including sex male OR: 3.55 [2.882; 4.598], p < 0.001, and cutoff points (age > 65, OR: 7.953 [7.256; 8.649], p < 0.001, NIHSS > 6, OR: 3.740 [2.882; 4.598], p < 0.01, and fibrinogen > 400 mg/dL, OR: 2.988 [2.290; 3.686], p < 0.01) showed a good global discrimination capability AUC = 0.89 (95%CI: 0.88–0.94).
Conclusions
In code stroke, a model including age, sex, NIHSS, and fibrinogen showed a good discrimination capability to differentiate between MA and Ischemic stroke. Whether these variables can be implemented in a diagnostic rule should be tested in future studies.



Similar content being viewed by others


Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Terrin A, Toldo G, Ermani M et al (2018) When migraine mimics stroke: a systematic review. Cephalalgia 38:2068–2078. https://doi.org/10.1177/0333102418767999
Keselman B, Cooray C, Vanhooren G et al (2019) Intravenous thrombolysis in stroke mimics: results from the SITS international stroke thrombolysis register. Eur J Neurol 26:1091–1097. https://doi.org/10.1111/ene.13944
Ali-Ahmed F, Federspiel JJ, Liang L et al (2019) Intravenous tissue plasminogen activator in stroke mimics: findings from the get with the guidelines-stroke registry. Circ Cardiovasc Qual Outcomes 12:1–9. https://doi.org/10.1161/CIRCOUTCOMES.119.005609
Kelman L (2004) The aura: a tertiary care study of 952 migraine patients. Cephalalgia 24:728–734. https://doi.org/10.1111/j.1468-2982.2004.00748.x
Gonzalez‐Martinez A, Trillo Senín S, Benavides Bernaldo de Queirós C, et al (2021) Clinical characteristics and perfusion‐computed tomography alterations in a series of patients with migraine with aura attended as stroke code. Headache: J Head Face Pain 61:1568–1574. https://doi.org/10.1111/head.14243
Ois A, Cuadrado-Godia E, Jiménez-Conde J et al (2007) Early arterial study in the prediction of mortality after acute ischemic stroke. Stroke 38:2085–2089. https://doi.org/10.1161/STROKEAHA.107.482950
Agència de Qualitat i Avaluació Sanitàries de Catalunya (2020) Registre Codi Ictus Catalunya. http://aquas.gencat.cat/ca/ambits/projectes/registre-cicat/resultats/cicat/. Accessed 10 Jan 2022
Sacco RL, Kasner SE, Broderick JP et al (2013) An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 44:2064–2089. https://doi.org/10.1161/STR.0b013e318296aeca
Olesen J (2018) Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 38:1–211. https://doi.org/10.1177/0333102417738202
Liberman AL, Liotta EM, Caprio FZ et al (2015) Do efforts to decrease door-to-needle time risk increasing stroke mimic treatment rates? Neurol Clin Pract 5:247–252. https://doi.org/10.1212/CPJ.0000000000000122
Burton TM, Luby M, Nadareishvili Z et al (2017) Effects of increasing IV tPA-treated stroke mimic rates at CT-based centers on clinical outcomes. Neurology 89:343–348. https://doi.org/10.1212/WNL.0000000000004149
Avellaneda-Gómez C, Rodríguez Campello A, Giralt Steinhauer E et al (2019) Description of stroke mimics after complete neurovascular assessment. Neurología (English Edition) 34:7–13. https://doi.org/10.1016/j.nrleng.2016.10.004
Stovner LJ, Nichols E, Steiner TJ et al (2018) Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol 17:954–976. https://doi.org/10.1016/S1474-4422(18)30322-3
Abbafati C, Abbas KM, Abbasi-Kangevari M et al (2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396:1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
Vongvaivanich K, Lertakyamanee P, Silberstein SD, Dodick DW (2015) Late-life migraine accompaniments: a narrative review. Cephalalgia 35:894–911. https://doi.org/10.1177/0333102414560635
Peng KP, Chen YT, Fuh JL et al (2017) Migraine and incidence of ischemic stroke: a nationwide population-based study. Cephalalgia 37:327–335. https://doi.org/10.1177/0333102416642602
Altamura C, Cascio Rizzo A, Viticchi G et al (2022) Shorter visual aura characterizes young and middle-aged stroke patients with migraine with aura. J Neurol 269:897–906. https://doi.org/10.1007/s00415-021-10671-x
Danesh J, Lewington S, Thompson SG et al (2005) Plasma fibrinogen level and the risk of major cardiovascular diseases and nonvascular mortality: an individual participant meta-analysis. J Am Med Assoc 294:1799–1809. https://doi.org/10.1001/jama.294.14.1799
Alpuente A, Gallardo VJ, Asskour L et al (2021) Salivary CGRP can monitor the different migraine phases: CGRP (in)dependent attacks. Cephalalgia. https://doi.org/10.1177/03331024211040467
Park JJ, Kim SJ, Kim HY et al (2020) Migraine with aura as a stroke mimic. Can J Neurol Sci 47:242–244. https://doi.org/10.1017/cjn.2019.316
Nieuwkamp DJ, Van Der Schaaf IC, Biessels GJ (2010) Migraine aura presenting as dysphasia with global cognitive dysfunction and abnormalities on perfusion CT. Cephalalgia 30:1007–1009. https://doi.org/10.1111/j.1468-2982.2009.02007.x
Hansen JM, Schytz HW, Larsen VA et al (2011) Hemiplegic migraine aura begins with cerebral hypoperfusion: imaging in the acute phase. Headache 51:1289–1296. https://doi.org/10.1111/j.1526-4610.2011.01963.x
Shah L, Rana S, Valeriano J, Scott TF (2013) Reversible CT perfusion abnormalities in patient with migraine variant: a two phase process. Clin Neurol Neurosurg 115:830–832. https://doi.org/10.1016/j.clineuro.2012.08.012
Miller C, Goldberg MF (2012) Susceptibility-weighted imaging and computed tomography perfusion abnormalities in diagnosis of classic migraine. Emerg Radiol 19:565–569. https://doi.org/10.1007/s10140-012-1051-2
Roth C, Ferbert A, Huegens-Penzel M et al (2018) Multimodal imaging findings during severe attacks of familial hemiplegic migraine type 2. J Neurol Sci 392:22–27. https://doi.org/10.1016/j.jns.2018.06.019
Hsu DA, Stafstrom CE, Rowley HA et al (2008) Hemiplegic migraine: hyperperfusion and abortive therapy with intravenous verapamil. Brain Dev 30:86–90. https://doi.org/10.1016/j.braindev.2007.05.013
Strambo D, Nannoni S, Rebordão L, et al (2022) Computed tomographic perfusion abnormalities in acute migraine with aura: characteristics and comparison with transient ischemic attack. Eur Stroke J 239698732211142. https://doi.org/10.1177/23969873221114256
Chalela JA, Kidwell CS, Nentwich LM et al (2007) Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet 369:293–298. https://doi.org/10.1016/S0140-6736(07)60151-2
Provost C, Soudant M, Legrand L et al (2019) Magnetic resonance imaging or computed tomography before treatment in acute ischemic stroke: effect on workflow and functional outcome. Stroke 50:659–664. https://doi.org/10.1161/STROKEAHA.118.023882
Lebedeva ER, Gurary NM, Gilev D, v, et al (2018) Explicit diagnostic criteria for transient ischemic attacks to differentiate it from migraine with aura. Cephalalgia 38:1463–1470. https://doi.org/10.1177/0333102417736901
Acknowledgements
We would like to thank Álvaro Villarino for his contribution to language edition of the manuscript.
Funding
This work was supported in part by Spain’s Ministry of Health (Instituto de Salud Carlos III, Fondos FEDER, RICORS-ICTUS (RD21/0006/0021)).
Author information
Authors and Affiliations
Contributions
AMG and ECG were involved in the conception and design of the study, interpretation of data, and in the writing of the manuscript. AMG and ASP contributed to data acquisition. ECG, AO, and JJB performed the statistical analysis. All authors interpreted the data, reviewed the manuscript, and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Macias-Gómez, A., Suárez-Pérez, A., Rodríguez-Campello, A. et al. Factors associated with migraine aura mimicking stroke in code stroke. Neurol Sci 44, 2113–2120 (2023). https://doi.org/10.1007/s10072-023-06641-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-023-06641-y