
Abstract
Objective
Sneddon’s syndrome is a cerebrocutaneous non-inflammatory progressive distal arteriopathy, characterized by livedo racemosa, stroke, and neuropsychiatric symptoms. Our aim was to highlight the characteristic neuroimaging features of Sneddon’s syndrome that might be helpful to clinicians in timely diagnosis of this entity.
Methods
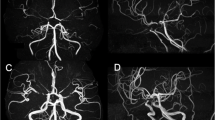
Twelve patients (median age 49 years, 11 female) with primary Sneddon’s syndrome, diagnosed in last 10 years, were analyzed from the perspective of magnetic resonance imaging (MRI) features. In addition, a novel pseudoangiomatosis score was defined for grading angiographic abnormalities (range: 0 to 6).
Results
Median interval from the onset of neurological symptoms to diagnosis was 6 years. Presentation was with acute stroke in 5, seizures in 3, dementia/speech problems in 2, seizures plus cognitive dysfunction in 1, and chronic progressive hemiparesis in 1. All patients had a typical lesion pattern on MRI. This included multiple (median 3) cortical-subcortical supratentorial and cerebellar non-territorial infarcts, accompanied by multifocal cerebral atrophy. Of note, large territorial infarcts due to cerebral parent artery occlusion, an embolic pattern with multi-territorial involvement on diffusion-weighted imaging, small vessel disease features like severe white matter involvement or lacunar infarcts, and cerebral hemorrhage in the absence of anticoagulation were not observed. MRI lesion severity was not correlated with angiographic arteriopathy severity, clinical stage, or presentation symptoms.
Conclusion
Sneddon’s syndrome is characterized by highly typical clinico-radiological features. Brain MRI has diagnostic value. By knowing the characteristics of the syndrome, misdiagnosis and potentially harmful treatment can be prevented in this entity that might pose a diagnostic challenge.




Similar content being viewed by others

Availability of data and material
If there is a need more than supplementary data already provided, all will be provided upon reasonable request.
References
Sneddon IB (1965) Cerebrovascular lesions and livedo reticularis. Br J Dermatol 77:180–185
Wu S, Xu Z, Liang H (2014) Sneddon's syndrome: a comprehensive review of the literature. Orphanet J Rare Dis 9:215. https://doi.org/10.1186/s13023-014-0215-4
Samanta D, Cobb S, Arya K (2019) Sneddon syndrome: a comprehensive overview. J Stroke Cerebrovasc Dis 28(8):2098–2108. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.05.013
Bottin L, Frances C, de Zuttere D, Boelle PY, Muresan IP, Alamowitch S (2015) Strokes in Sneddon syndrome without antiphospholipid antibodies. Ann Neurol 77(5):817–829. https://doi.org/10.1002/ana.24382
Zelger B, Sepp N, Stockhammer G, Dosch E, Hilty E, Ofner D, Aichner F, Fritsch PO (1993) Sneddon's syndrome. A long-term follow-up of 21 patients. Arch Dermatol 129(4):437–447. https://doi.org/10.1001/archderm.129.4.437
Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, Lindley RI, O'Brien JT, Barkhof F, Benavente OR, Black SE, Brayne C, Breteler M, Chabriat H, Decarli C, de Leeuw FE, Doubal F, Duering M, Fox NC, Greenberg S, Hachinski V, Kilimann I, Mok V, Oostenbrugge R, Pantoni L, Speck O, Stephan BC, Teipel S, Viswanathan A, Werring D, Chen C, Smith C, van Buchem M, Norrving B, Gorelick PB, Dichgans M, nEuroimaging STfRVco (2013) Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol 12(8):822–838. https://doi.org/10.1016/S1474-4422(13)70124-8
Buyukserbetci G, Saka E, Oguz KK, Gocmen R, Arsava EM, Topcuoglu MA (2018) Cognitive dysfunction in relation to topography and burden of cerebral microbleeds. Noro Psikiyatr Ars 55(1):84–90. https://doi.org/10.29399/npa.23018
Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA (1987) MR signal abnormalities at 1.5 T in Alzheimer's dementia and normal aging. AJR Am J Roentgenol 149(2):351–356. https://doi.org/10.2214/ajr.149.2.351
Farrell C, Chappell F, Armitage PA, Keston P, Maclullich A, Shenkin S, Wardlaw JM (2009) Development and initial testing of normal reference MR images for the brain at ages 65-70 and 75-80 years. Eur Radiol 19(1):177–183. https://doi.org/10.1007/s00330-008-1119-2
Marinho JL, Piovesan EJ, Leite Neto MP, Kotze LR, Noronha L, Twardowschy CA, Lange MC, Scola RH, Zetola VH, Novak EM, Werneck LC (2007) Clinical, neurovascular and neuropathological features in Sneddon's syndrome. Arq Neuropsiquiatr 65(2B):390–395. https://doi.org/10.1590/s0004-282x2007000300005
Cavestro C, Richetta L, Pedemonte E, Asteggiano G (2009) Sneddon's syndrome presenting with severe disabling bilateral headache. J Headache Pain 10(3):211–213. https://doi.org/10.1007/s10194-009-0109-3
Killeen T, Wanke I, Mangiardi J, Cesnulis E (2014) Ruptured, fusiform, distal lenticulostriate aneurysm causing intraventricular haemorrhage in a patient with antiphospholipid-negative Sneddon's syndrome. Clin Neurol Neurosurg 116:80–82. https://doi.org/10.1016/j.clineuro.2013.11.009
Amarenco P, Levy C, Cohen A, Touboul PJ, Roullet E, Bousser MG (1994) Causes and mechanisms of territorial and nonterritorial cerebellar infarcts in 115 consecutive patients. Stroke 25(1):105–112. https://doi.org/10.1161/01.str.25.1.105
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Waived for this analysis. Stroke database and its protocols were approved by university ethical committee.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(PDF 567 kb)
Rights and permissions
About this article

Cite this article
Yilmaz, E., Arsava, E.M., Gocmen, R. et al. Characteristic imaging features of neurovascular involvement in primary Sneddon’s syndrome: an analysis of 12 cases. Neurol Sci 42, 2363–2369 (2021). https://doi.org/10.1007/s10072-020-04621-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-020-04621-0