
Abstract
Background
Osteophyte formation is an important radiographic sign of osteoarthritis (OA) and limited joint motion in knee osteoarthritis patients. Some studies revealed relationships of osteophyte formation with a high bone mineral density and a high muscle mass, while others showed no correlations. The aim of this study was to identify relationships of osteophyte formation with bone mineral density and muscle mass.
Methods
A cross sectional study of knee osteoarthritis was conducted. Cases were classified as patients with osteophyte formation, while controls were those without osteophytes. All subjects underwent a knee x-ray and bone mineral density and body composition evaluation. General patient characteristics, covariates, and the results of biochemical analyses were also recorded. Statistical analysis was conducted using SPSS Version 22.0. Logistic regression and the chi-square test were utilized to analyze the relationships between the presence of knee osteophytes and the study variables.
Results
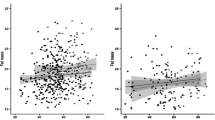
A total of 228 patients were enrolled, including 78 with osteophytes in the knee joint and 150 without. A total of 162/228 are females; knee OA is commonly explained among females. (p = 0.001). The mean age was 73.23 ± 11.10 years in the osteophyte group and 71.86 ± 12.23 in the no osteophyte group (p = 0.409). The mean body mass index was 24.15 ± 3.27 kg/m2 in the osteophyte group and 23.37 ± 3.48 kg/m2 in the no osteophyte group (p = 0.433). More patients in the osteophyte group had hypertension (p = 0.002), so the age group 73 years expected to have OA and hypertension along other metabolic diseases, and the femoral neck T score was higher in the osteophyte group (p = 0.044). Logistic regression analysis showed that the male gender was associated with less osteophyte formation (p = 0.001, odds ratio (OR) 0.11 (0.03–0.37)), and hypertension was associated with increased muscle loss (p = 0.005). Femoral neck T score was associated with the presence of osteophyte formation (p = 0.011, OR 1.98 (1.17–3.36)).
Conclusions
The results demonstrated an association of knee osteophyte formation with the femoral neck T score and hypertension, but no association with muscle mass. We speculated that in patients with osteophytosis and increased bone mass, metabolic factors such as hypertension should be considered. Further study of the molecular mechanisms regulating these processes is needed in the future.
Key Points • Associations of knee osteophyte formation with the femoral neck T score, but not with muscle mass. • Those with osteophytosis and an increased bone mass and metabolic factors such as hypertension need to be assessed. |
Similar content being viewed by others

Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- OA:
-
Osteoarthritis
- BMD:
-
Bone mineral density
- ACR:
-
American College of Rheumatology
- DXA:
-
Dual-energy X-ray absorptiometry
References
Kijowski R, Blankenbaker DG, Stanton PT, Fine JP, De Smet AA (2006) Radiographic findings of osteoarthritis versus arthroscopic findings of articular cartilage degeneration in the tibiofemoral joint. Radiology 239(3):818–824
van der Kraan PM, van den Berg WB (2007) Osteophytes: relevance and biology. Osteoarthritis Cartilage 15(3):237–244
Burger H, van Daele PL, Odding E, Valkenburg HA, Hofman A, Grobbee DE et al (1996) Association of radiographically evident osteoarthritis with higher bone mineral density and increased bone loss with age. Rotterdam Study Arthritis Rheum 39(1):81–86
Nevitt MC, Lane NE, Scott JC, Hochberg MC, Pressman AR, Genant HK, et al. (1995) Radiographic osteoarthritis of the hip and bone mineral density. The Study of Osteoporotic Fractures Research Group. Arthritis Rheum 38(7):907–16
Hannan MT, Anderson JJ, Zhang Y, Levy D, Felson DT (1993) Bone mineral density and knee osteoarthritis in elderly men and women. Framingham Study Arthritis Rheum 36(12):1671–1680
Hochberg MC (2004) Do risk factors for incident hip osteoarthritis (OA) differ from those for progression of hip OA? J Rheumatol Suppl 70:6–9
Dequeker J, Boonen S, Aerssens J, Westhovens R (1996) Inverse relationship osteoarthritis-osteoporosis: what is the evidence? What are the consequences? Br J Rheumatol 35(9):813–818
El-Sherif HE, Kamal R, Moawyah O (2008) Hand osteoarthritis and bone mineral density in postmenopausal women; clinical relevance to hand function, pain and disability. Osteoarthr Cartil 16(1):12–17
Hochberg MC, Lethbridge-Cejku M, Tobin JD (2004) Bone mineral density and osteoarthritis: data from the Baltimore Longitudinal Study of Aging. Osteoarthr Cartil 12 Suppl A:S45–8.
Schneider DL, Barrett-Connor E, Morton DJ, Weisman M (2002) Bone mineral density and clinical hand osteoarthritis in elderly men and women: the Rancho Bernardo study. J Rheumatol 29(7):1467–1472
Zoli A, Lizzio MM, Capuano A, Massafra U, Barini A, Ferraccioli G (2006) Osteoporosis and bone metabolism in postmenopausal women with osteoarthritis of the hand. Menopause 13(3):462–466
Milte R, Crotty M (2014) Musculoskeletal health, frailty and functional decline. Best Pract Res Clin Rheumatol 28(3):395–410
Kemmler W, Teschler M, Goisser S, Bebenek M, von Stengel S, Bollheimer LC et al (2015) Prevalence of sarcopenia in Germany and the corresponding effect of osteoarthritis in females 70 years and older living in the community: results of the FORMoSA study. Clin Interv Aging 10:1565–1573
Conroy MB, Kwoh CK, Krishnan E, Nevitt MC, Boudreau R, Carbone LD et al (2012) Muscle strength, mass, and quality in older men and women with knee osteoarthritis. Arthritis Care Res (Hoboken) 64(1):15–21
Waters RL, Campbell J, Perry J (1987) Energy cost of three-point crutch ambulation in fracture patients. J Orthop Trauma 1(2):170–173
Papalia R, Zampogna B, Torre G, Lanotte A, Vasta S, Albo E et al (2014) Sarcopenia and its relationship with osteoarthritis: risk factor or direct consequence? Musculoskelet Surg 98(1):9–14
Kellgren JH, Lawrence JS (1957) Radiological assessment of osteo-arthrosis. Ann Rheum Dis 16(4):494–502
Ho-Pham LT, Lai TQ, Mai LD, Doan MC, Pham HN, Nguyen TV (2014) Prevalence of radiographic osteoarthritis of the knee and its relationship to self-reported pain. PLoS One 9(4):e94563
Celi M, Rao C, Scialdoni A, Tempesta V, Gasbarra E, Pistillo P et al (2013) Bone mineral density evaluation in osteoporosis: why yes and why not? Aging Clin Exp Res 25(Suppl 1):S47–S49
Gregson CL, Sayers A, Lazar V, Steel S, Dennison EM, Cooper C et al (2013) The high bone mass phenotype is characterised by a combined cortical and trabecular bone phenotype: findings from a pQCT case-control study. Bone 52(1):380–388
Hardcastle SA, Gregson CL, Deere KC, Davey Smith G, Dieppe P, Tobias JH (2013) High bone mass is associated with an increased prevalence of joint replacement: a case-control study. Rheumatology (Oxford) 52(6):1042–1051
Gregson CL, Paggiosi MA, Crabtree N, Steel SA, McCloskey E, Duncan EL et al (2013) Analysis of body composition in individuals with high bone mass reveals a marked increase in fat mass in women but not men. J Clin Endocrinol Metab 98(2):818–828
Felson DT, Neogi T (2004) Osteoarthritis: is it a disease of cartilage or of bone? Arthritis Rheum 50(2):341–344
Rogers J, Shepstone L, Dieppe P (1997) Bone formers: osteophyte and enthesophyte formation are positively associated. Ann Rheum Dis 56(2):85–90
De Ceuninck F, Fradin A, Pastoureau P (2014) Bearing arms against osteoarthritis and sarcopenia: when cartilage and skeletal muscle find common interest in talking together. Drug Discov Today 19(3):305–311
Yoshimura N, Muraki S, Oka H, Kawaguchi H, Nakamura K, Akune T (2011) Association of knee osteoarthritis with the accumulation of metabolic risk factors such as overweight, hypertension, dyslipidemia, and impaired glucose tolerance in Japanese men and women: the ROAD study. J Rheumatol 38(5):921–930
Xie DX, Wei J, Zeng C, Yang T, Li H, Wang YL et al (2017) Association between metabolic syndrome and knee osteoarthritis: a cross-sectional study. BMC Musculoskelet Disord 18(1):533
Kang X, Fransen M, Zhang Y, Li H, Ke Y, Lu M et al (2009) The high prevalence of knee osteoarthritis in a rural Chinese population: the Wuchuan osteoarthritis study. Arthritis Rheum 61(5):641–647
Salve H, Gupta V, Palanivel C, Yadav K, Singh B (2010) Prevalence of knee osteoarthritis amongst perimenopausal women in an urban resettlement colony in South Delhi. Indian J Public Health 54(3):155–157
Nestel P, Lyu R, Low LP, Sheu WH, Nitiyanant W, Saito I et al (2007) Metabolic syndrome: recent prevalence in East and Southeast Asian populations. Asia Pac J Clin Nutr 16(2):362–367
Gandhi R, Razak F, Tso P, Davey JR, Mahomed NN (2010) Asian ethnicity and the prevalence of metabolic syndrome in the osteoarthritic total knee arthroplasty population. J Arthroplasty 25(3):416–419
Sowers M, Karvonen-Gutierrez CA, Palmieri-Smith R, Jacobson JA, Jiang Y, Ashton-Miller JA (2009) Knee osteoarthritis in obese women with cardiometabolic clustering. Arthritis Rheum 61(10):1328–1336
Kornaat PR, Sharma R, van der Geest RJ, Lamb HJ, Kloppenburg M, Hellio le Graverand MP, et al. (2009) Positive association between increased popliteal artery vessel wall thickness and generalized osteoarthritis: is OA also part of the metabolic syndrome? Skeletal Radiol 38(12):1147–51
Rojas-Rodriguez J, Escobar-Linares LE, Garcia-Carrasco M, Escarcega RO, Fuentes-Alexandro S, Zamora-Ustaran A (2007) The relationship between the metabolic syndrome and energy-utilization deficit in the pathogenesis of obesity-induced osteoarthritis. Med Hypotheses 69(4):860–868
Cai H, Sun HJ, Wang YH, Zhang Z (2015) Relationships of common polymorphisms in IL-6, IL-1A, and IL-1B genes with susceptibility to osteoarthritis: a meta-analysis. Clin Rheumatol 34(8):1443–1453
Lukic L, Lalic NM, Rajkovic N, Jotic A, Lalic K, Milicic T et al (2014) Hypertension in obese type 2 diabetes patients is associated with increases in insulin resistance and IL-6 cytokine levels: potential targets for an efficient preventive intervention. Int J Environ Res Public Health 11(4):3586–3598
Lanyon P, Muir K, Doherty S, Doherty M (2003) Age and sex differences in hip joint space among asymptomatic subjects without structural change: implications for epidemiologic studies. Arthritis Rheum 48(4):1041–1046
Funding
This study was supported by Chang Gung Memorial Hospital and Chang Gung University College of Medicine (CMRPG8H0521). The funders had no role in study design, data collection and analysis, decision to publish, nor preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
KTW: study design, data collection, statistical analysis, and writing the paper; TTC: data collection; RWW, CCH: study design and writing the paper; YCC: corresponding author, study design, and writing the paper. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and with approval by the Institutional Review Board of Chang Gung Memorial Hospital, IRB No.: 201800414A3. Informed consent was obtained from the individuals who had joined the study.
Consent for publication
Informed written consent was provided by every participant.
Disclosures
None.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wu, KT., Wang, YW., Wu, RW. et al. Association of a femoral neck T score with knee joint osteophyte formation but not with skeletal muscle mass. Clin Rheumatol 42, 917–922 (2023). https://doi.org/10.1007/s10067-022-06410-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-022-06410-w