
Abstract
Introduction/objectives
Hyponatremia is a potential risk factor for the development of coronary artery lesions (CALs) identified after acute Kawasaki disease (KD). However, the serum sodium distribution corresponding to the reference intervals differs between infants (< 1 year of age) and older children. We hypothesized the association of serum sodium level with CAL complications differs between infants and older patients with KD.
Methods
We analyzed 21,610 population-based patients who developed KD throughout Japan during 2013–2014. We performed multivariable logistic regression analyses to evaluate the association between serum sodium and CAL complications. Additionally, we stratified the serum sodium distribution associated with CAL complications by infants and older patients.
Results
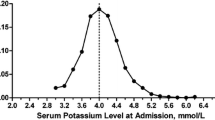
CALs were identified in 158 (3.6%) infants and 302 (1.8%) older patients. Infants were more likely to develop CALs when within the normal sodium range compared with older patients (75% vs. 29%), whereas most older patients developed CALs with a sodium level lower than the reference interval. Serum sodium ≤ 130 mEq/L indicated significantly higher risk for development of CALs in both groups (adjusted odds ratio [95% confidence intervals] = 3.21 [1.65–6.25] in infants and 1.74 [1.18–2.57] in older patients).
Conclusions
Serum sodium distribution associated with CAL complications differed greatly between infants and older patients. Older patients developed CALs with sodium levels lower than the reference interval; however, among infants, hyponatremia was not necessarily a risk factor for developing coronary artery lesion. When considering risk assessments for CALs using serum sodium levels, infants with KD should be distinguished from older patients.
Key Points • Hyponatremia is a potential risk factor for the development of coronary artery lesions (CALs) among patients with Kawasaki disease. • However, the serum sodium distribution corresponding to the reference intervals differs between infants (< 1 year of age) and older children. • Most infants developed CALs within the normal sodium range, whereas older patients developed at a range lower than the reference interval. • These findings highlight that when considering risk assessments for CALs using serum sodium levels, infants should be distinguished from older patients. |




Similar content being viewed by others


Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
McCrindle BW, Rowley AH, Newburger JW et al (2017) Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation 135:e927–e999. https://doi.org/10.1161/CIR.0000000000000484
Newburger JW, Takahashi M, Beiser AS et al (1991) A single intravenous infusion of gamma globulin as compared with four infusions in the treatment of acute Kawasaki syndrome. N Engl J Med 324:1633–1639. https://doi.org/10.1056/nejm199106063242305
Furusho K, Kamiya T, Nakano H et al (1984) High-dose intravenous gammaglobulin for Kawasaki disease. Lancet 2:1055–1058
Ae R, Makino N, Kosami K, Kuwabara M, Matsubara Y, Nakamura Y (2020) Epidemiology, treatments, and cardiac complications in patients with Kawasaki disease: the nationwide survey in Japan, 2017–2018. J Pediatr 225:23-29.e22. https://doi.org/10.1016/j.jpeds.2020.05.034
Uehara R, Belay ED, Maddox RA et al (2008) Analysis of potential risk factors associated with nonresponse to initial intravenous immunoglobulin treatment among Kawasaki disease patients in Japan. Pediatr Infect Dis J 27:155–160. https://doi.org/10.1097/INF.0b013e31815922b5
Ae R, Abrams JY, Maddox RA et al (2020) Outcomes in Kawasaki disease patients with coronary artery abnormalities at admission. Am Heart J 225:120–128. https://doi.org/10.1016/j.ahj.2020.04.019
Laxer RM, Petty RE (1982) Hyponatremia in Kawasaki disease. Pediatrics 70:655
Watanabe T, Abe Y, Sato S, Uehara Y, Ikeno K, Abe T (2006) Hyponatremia in Kawasaki disease. Pediatr Nephrol 21:778–781. https://doi.org/10.1007/s00467-006-0086-6
Fernandez-Cooke E, Barrios Tascón A, Sánchez-Manubens J et al (2019) Epidemiological and clinical features of Kawasaki disease in Spain over 5 years and risk factors for aneurysm development. (2011–2016): KAWA-RACE study group. PLoS One 14(5):e0215665. https://doi.org/10.1371/journal.pone.0215665
Hashimoto I (2019) Indicators of unresponsiveness after initial i.v. immunoglobulin treatment in acute Kawasaki disease. Pediatr Int 61:641–646. https://doi.org/10.1111/ped.13898
Tan XH, Zhang XW, Wang XY et al (2019) A new model for predicting intravenous immunoglobin-resistant Kawasaki disease in Chongqing: a retrospective study on 5277 patients. Sci Rep 9:1722. https://doi.org/10.1038/s41598-019-39330-y
Wu S, Long Y, Chen S et al (2019) A new scoring system for prediction of intravenous immunoglobulin resistance of Kawasaki disease in infants under 1-year old. Front Pediatr 7:514. https://doi.org/10.3389/fped.2019.00514
Yang S, Song R, Zhang J, Li X, Li C (2019) Predictive tool for intravenous immunoglobulin resistance of Kawasaki disease in Beijing. Arch Dis Child 104:262–267. https://doi.org/10.1136/archdischild-2017-314512
Kobayashi T, Inoue Y, Takeuchi K et al (2006) Prediction of intravenous immunoglobulin unresponsiveness in patients with Kawasaki disease. Circulation 113:2606–2612. https://doi.org/10.1161/circulationaha.105.592865
Egami K, Muta H, Ishii M et al (2006) Prediction of resistance to intravenous immunoglobulin treatment in patients with Kawasaki disease. J Pediatr 149:237–240. https://doi.org/10.1016/j.jpeds.2006.03.050
Sano T, Kurotobi S, Matsuzaki K et al (2007) Prediction of non-responsiveness to standard high-dose gamma-globulin therapy in patients with acute Kawasaki disease before starting initial treatment. Eur J Pediatr 166:131–137. https://doi.org/10.1007/s00431-006-0223-z
Ae R, Abrams JY, Maddox RA et al (2020) Corticosteroids added to initial intravenous immunoglobulin treatment for the prevention of coronary artery abnormalities in high-risk patients with Kawasaki disease. J Am Heart Assoc 9:e015308. https://doi.org/10.1161/jaha.119.015308
Tremoulet AH (2018) Adjunctive therapies in Kawasaki disease. Int J Rheum Dis 21:76–79. https://doi.org/10.1111/1756-185x.13208
Miyata K, Kaneko T, Morikawa Y et al (2018) Efficacy and safety of intravenous immunoglobulin plus prednisolone therapy in patients with Kawasaki disease (Post RAISE): a multicentre, prospective cohort study. Lancet Child Adolesc Health 2:855–862. https://doi.org/10.1016/s2352-4642(18)30293-1
Kobayashi T, Saji T, Otani T et al (2012) Efficacy of immunoglobulin plus prednisolone for prevention of coronary artery abnormalities in severe Kawasaki disease (RAISE study): a randomised, open-label, blinded-endpoints trial. Lancet 379:1613–1620. https://doi.org/10.1016/s0140-6736(11)61930-2
Chen S, Dong Y, Kiuchi MG et al (2016) Coronary artery complication in Kawasaki disease and the importance of early intervention : a systematic review and meta-analysis. JAMA Pediatr 170:1156–1163. https://doi.org/10.1001/jamapediatrics.2016.2055
Chen S, Dong Y, Yin Y, Krucoff MW (2013) Intravenous immunoglobulin plus corticosteroid to prevent coronary artery abnormalities in Kawasaki disease: a meta-analysis. Heart 99:76–82. https://doi.org/10.1136/heartjnl-2012-302126
Dean B. Andropoulos MD M. Appendix B: pediatric normal laboratory values. George’s Pediatric Anesthesia. 2012(Fifth edition):1300–1314
Chantasiriwan N, Silvilairat S, Makonkawkeyoon K, Pongprot Y, Sittiwangkul R (2018) Predictors of intravenous immunoglobulin resistance and coronary artery aneurysm in patients with Kawasaki disease. Paediatr Int Child Health 38:209–212. https://doi.org/10.1080/20469047.2018.1471381
Davies S, Sutton N, Blackstock S et al (2015) Predicting IVIG resistance in UK Kawasaki disease. Arch Dis Child 100:366–368. https://doi.org/10.1136/archdischild-2014-307397
Jakob A, von Kries R, Horstmann J et al (2018) Failure to predict high-risk Kawasaki disease patients in a population-based study cohort in Germany. Pediatr Infect Dis J 37:850–855. https://doi.org/10.1097/inf.0000000000001923
Sleeper LA, Minich LL, McCrindle BM et al (2011) Evaluation of Kawasaki disease risk-scoring systems for intravenous immunoglobulin resistance. J Pediatr 158:831-835.e833. https://doi.org/10.1016/j.jpeds.2010.10.031
Makino N, Nakamura Y, Yashiro M et al (2018) Epidemiological observations of Kawasaki disease in Japan, 2013–2014. Pediatr Int 60:581–587. https://doi.org/10.1111/ped.13544
Guidelines for medical treatment of acute Kawasaki disease: report of the Research Committee of the Japanese Society of Pediatric Cardiology and Cardiac Surgery; (2012) revised version (2014). Pediatr Int 56:135–158. https://doi.org/10.1111/ped.12317
Ayusawa M, Sonobe T, Uemura S et al (2005) Revision of diagnostic guidelines for Kawasaki disease (the 5th revised edition). Pediatr Int 47(2):232–234. https://doi.org/10.1111/j.1442-200x.2005.02033.x
JCS Joint Working Group (2014) Guidelines for diagnosis and management of cardiovascular sequelae in Kawasaki disease (JCS 2013). Digest version Circ J 78:2521–2562. https://doi.org/10.1253/circj.cj-66-0096
Akagi T, Rose V, Benson LN, Newman A, Freedom RM (1992) Outcome of coronary artery aneurysms after Kawasaki disease. J Pediatr 121:689–694. https://doi.org/10.1016/S0022-3476(05)81894-3
Muta H, Ishii M, Egami K et al (2005) Serum sodium levels in patients with Kawasaki disease. Pediatr Cardiol 26:404–407. https://doi.org/10.1007/s00246-004-0789-z
Nakamura Y, Yashiro M, Uehara R et al (2004) Use of laboratory data to identify risk factors of giant coronary aneurysms due to Kawasaki disease. Pediatr Int 46:33–38. https://doi.org/10.1111/j.1442-200X.2004.01840.x
Cameron SA, Carr M, Pahl E, DeMarais N, Shulman ST, Rowley AH (2019) Coronary artery aneurysms are more severe in infants than in older children with Kawasaki disease. Arch Dis Child 104:451–455. https://doi.org/10.1136/archdischild-2018-314967
Salgado AP, Ashouri N, Berry EK et al (2017) High risk of coronary artery aneurysms in infants younger than 6 months of age with Kawasaki disease. J Pediatr 185:112-116.e111. https://doi.org/10.1016/j.jpeds.2017.03.025
Miura K, Harita Y, Takahashi N et al (2020) Nonosmotic secretion of arginine vasopressin and salt loss in hyponatremia in Kawasaki disease. Pediatr Int 62:363–370. https://doi.org/10.1111/ped.14036
Kil HR (2010) Kawasaki disease and hyponatremia. Korean Circ J 40:489–490. https://doi.org/10.4070/kcj.2010.40.10.489
Lim GW, Lee M, Kim HS, Hong YM, Sohn S (2010) Hyponatremia and syndrome of inappropriate antidiuretic hormone secretion in kawasaki disease. Korean Circ J 40:507–513. https://doi.org/10.4070/kcj.2010.40.10.507
Mori J, Miura M, Shiro H, Fujioka K, Kohri T, Hasegawa T (2011) Syndrome of inappropriate anti-diuretic hormone in Kawasaki disease. Pediatr Int 53:354–357. https://doi.org/10.1111/j.1442-200X.2010.03264.x
Dionne A, Burns JC, Dahdah N et al (2019) Treatment intensification in patients with Kawasaki disease and coronary aneurysm at diagnosis. Pediatrics 143:e20183341. https://doi.org/10.1542/peds.2018-3341
de Zorzi A, Colan SD, Gauvreau K, Baker AL, Sundel RP, Newburger JW (1998) Coronary artery dimensions may be misclassified as normal in Kawasaki disease. J Pediatr 133:254–258
Burns JC, Hoshino S, Kobayashi T (2018) Kawasaki disease: an essential comparison of coronary artery aneurysm criteria. Lancet Child Adolesc Health 2:840–841. https://doi.org/10.1016/s2352-4642(18)30334-1
Belay ED, Maddox RA, Holman RC, Curns AT, Ballah K, Schonberger LB (2006) Kawasaki syndrome and risk factors for coronary artery abnormalities: United States, 1994–2003. Pediatr Infect Dis J 25:245–249. https://doi.org/10.1097/01.inf.0000202068.30956.16
Acknowledgements
We thank all the pediatricians who contributed to the nationwide survey of Kawasaki disease in Japan. The study was partially supported by grants and funding from a non-profit organization, The Japan Kawasaki Disease Research Center. We thank J. Ludovic Croxford, PhD, from Edanz Group (https://en-author-services.edanz.com/ac) for editing a draft of this manuscript.
Funding
The study was partially supported by grants and funding from a non-profit organization, the Japan Kawasaki Disease Research Center.
Author information
Authors and Affiliations
Contributions
HM: conceptualization, formal analysis, literature review, investigation, software, writing—original draft. RA: conceptualization, data curation, formal analysis, literature review, investigation, software, writing—original draft and review and editing. TK: formal analysis, investigation, methodology, software. MM: supervision, final approval. KK: formal analysis, investigation, methodology, software. KH: formal analysis, investigation, methodology, software. NM: data curation, supervision. YM: data curation, formal analysis. TS: data curation, Supervision. YN: funding acquisition, conceptualization, investigation, methodology, project administration, supervision, writing—review and editing, final approval.
Corresponding author
Ethics declarations
Ethics approval
The Jichi Medical University Clinical Research Ethics Committee approved the study and waived the requirement for informed consent from each participant (Approval ID: 18–070).
Consent for publication
All of the authors contributed significantly to the work, approved the manuscript, and agree with its submission and publication.
Conflict of interest
Dr. Nakamura has received grants and funding from a non-profit organization, the Japan Kawasaki Disease Research Center. The other authors have no conflicts of interest to declare.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Ryusuke Ae contributed equally as the co-first author.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Masuda, H., Ae, R., Koshimizu, Ta. et al. Serum sodium level associated with coronary artery lesions in patients with Kawasaki disease. Clin Rheumatol 41, 137–145 (2022). https://doi.org/10.1007/s10067-021-05881-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-021-05881-7