
Abstract
Objective
Bone sarcoidosis is usually rare. Imaging procedures such as fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) can reveal bone sarcoidosis with better sensitivity than conventional radiography. We aimed to describe bone sarcoidosis involvement detected with 18F-FDG PET/CT.
Methods
This was an observational retrospective study of individuals with pulmonary sarcoidosis who underwent 18F-FDG PET/CT. According to the ATS/ERS/WASOG criteria, sarcoidosis was diagnosed by the presence of clinical and/or imaging features of sarcoidosis and evidence of non-caseating epithelioid granulomas on a biopsy. We assessed clinical and 18F-FDG PET/CT characteristics.
Results
Data for 85 patients with sarcoidosis (56.5% female, median age 47 [range 21–80] years) were analyzed. The median follow-up was 4 years. Among 56 patients, sarcoidosis occurred in more than three organs. According to ATS/ERS/WASOG criteria, bone sarcoidosis was diagnosed in 12 (14%) patients. The spine was the most commonly affected location (92%, n = 11), followed by the pelvis (67%, n = 8), sternum (33%, n = 4), humerus (25%, n = 3), and fingers (17%, n = 2). Only peripheral adenopathy was associated with bone sarcoidosis (p = 0.04). Seven patients had a 18F-FDG PET/CT follow-up, all showing a decrease of bone lesions.
Conclusion
Bone sarcoidosis occurred in 14% of patients with sarcoidosis, affecting multiple bones and mostly the axial skeleton. 18F-FDG PET/CT seems a sensitive tool for diagnosis and follow-up of bone sarcoidosis.
Key Points • Bone sarcoidosis is not rare. • Bone sarcoidosis affects mainly the axial skeleton. • 18F-FDG PET/CT is useful for diagnosis and follow-up of bone sarcoidosis. |


Similar content being viewed by others


References
Lefere M, Larbi A, Malghem J, Berg BV, Dallaudière B (2014) Vertebral sarcoidosis: long-term follow-up with MRI. Skelet Radiol 43:1185–1190. https://doi.org/10.1007/s00256-014-1870-1
Bechman K, Christidis D, Walsh S, Birring SS, Galloway J (2018) A review of the musculoskeletal manifestations of sarcoidosis. Rheumatology (Oxford) 57:777–783. https://doi.org/10.1093/rheumatology/kex317
Thelier N, Assous N, Job-Deslandre C, Meyer O, Bardin T, Orcel P, Lioté F, Dougados M, Kahan A, Allanore Y (2008) Osteoarticular involvement in a series of 100 patients with sarcoidosis referred to rheumatology departments. J Rheumatol 35:1622–1628
Conte G, Zugni F, Colleoni M, Renne G, Bellomi M, Petralia G (2015) Sarcoidosis with bone involvement mimicking metastatic disease at 18F-FDG PET/CT: problem solving by diffusion whole-body MRI. Ecancermedicalscience 9. https://doi.org/10.3332/ecancer.2015.537
Sparks JA, McSparron JI, Shah N, Aliabadi P, Paulson V, Fanta CH, Coblyn JS (2014) Osseous sarcoidosis: clinical characteristics, treatment, and outcomes—experience from a large, academic hospital. Semin Arthritis Rheum 44:371–379. https://doi.org/10.1016/j.semarthrit.2014.07.003
Wilcox A, Bharadwaj P, Sharma OP (2000) Bone sarcoidosis. Curr Opin Rheumatol 12:321
Zhou Y, Lower EE, Li H, Farhey Y, Baughman RP (2017) Clinical characteristics of patients with bone sarcoidosis. Semin Arthritis Rheum 47. https://doi.org/10.1016/j.semarthrit.2017.02.004
Glaudemans AWJM, Vries D, Filippo JE, Galli F, Dierckx RAJO, Slart RHJA et al (2013) The use of F-FDG-PET/CT for diagnosis and treatment monitoring of inflammatory and infectious diseases. J Immunol Res. https://doi.org/10.1155/2013/623036
Aberg C, Ponzo F, Raphael B, Amorosi E, Moran V, Kramer E (2004) FDG positron emission tomography of bone involvement in sarcoidosis. AJR Am J Roentgenol 182:975–977. https://doi.org/10.2214/ajr.182.4.1820975
Baldini S, Pupi A, Di Lollo S, Marchionni N, Shraim R, Bosi A (2008) PET positivity with bone marrow biopsy revealing sarcoidosis in a patient in whom bone marrow metastases had been suspected. Br J Haematol 143:306. https://doi.org/10.1111/j.1365-2141.2008.07288.x
Clarençon F, Silbermann-Hoffman O, Lebreton C, Fernandez P, Kerrou K, Marchand-Adam S, Hourseau M, Schouman-Claeys E, Feydy A (2007) Diffuse spine involvement in sarcoidosis with sternal lytic lesions: two case reports. Spine 32:E594–E597. https://doi.org/10.1097/BRS.0b013e31814b86d5
Grozdic Milojevic I, Sobic-Saranovic D, Videnovic-Ivanov J, Saranovic D, Odalovic S, Artiko V (2016) FDG PET/CT in bone sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis 33:66–74
Kaira K, Oriuchi N, Otani Y, Yanagitani N, Sunaga N, Hisada T, Ishizuka T, Endo K, Mori M (2007) Diagnostic usefulness of fluorine-18-alpha-methyltyrosine positron emission tomography in combination with 18F-fluorodeoxyglucose in sarcoidosis patients. Chest 131:1019–1027. https://doi.org/10.1378/chest.06-2160
Ludwig V, Fordice S, Lamar R, Martin WH, Delbeke D (2003) Unsuspected skeletal sarcoidosis mimicking metastatic disease on FDG positron emission tomography and bone scintigraphy. Clin Nucl Med 28:176–179. https://doi.org/10.1097/01.RLU.0000053528.35645.70
Mostard RL, Prompers L, Weijers RE, van Kroonenburgh MJ, Wijnen PA, Geusens PP, Drent M (2012) F-18 FDG PET/CT for detecting bone and bone marrow involvement in sarcoidosis patients. Clin Nucl Med 37:21–25. https://doi.org/10.1097/RLU.0b013e3182335f9b
de Prost N, Kerrou K, Sibony M, Talbot J-N, Wislez M, Cadranel J (2010) Fluorine-18 Fluorodeoxyglucose with positron emission tomography revealed bone marrow involvement in Sarcoidosis patients with Anaemia. RES 79:25–31. https://doi.org/10.1159/000204901
Costabel U, Hunninghake GW (1999) ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis statement committee. American Thoracic Society. European Respiratory Society. World Association for Sarcoidosis and Other Granulomatous Disorders. Eur Respir J 14:735–737
Judson MA, Costabel U, Drent M, Wells A, Maier L, Koth L et al (2014) The WASOG Sarcoidosis organ assessment instrument: an update of a previous clinical tool. Sarcoidosis Vasc Diffuse Lung Dis 31:19–27
James DG, Neville E, Siltzbach LE (1976) A worldwide review of sarcoidosis. Ann N Y Acad Sci 278:321–334
Zisman DA, Shorr AF, Lynch JP (2002) Sarcoidosis involving the musculoskeletal system. Semin Respir Crit Care Med 23:555–570. https://doi.org/10.1055/s-2002-36520
Acknowledgments
We thank Laura Smales (BioMedEditing) for copyediting.
b X-rays of fingers. Presence of an enlargement of the feeder holes (asterisk) of phalanges associated with a mesh appearance (long white arrow), acro-osteolysis (circle), pseudocystic lesions eroding the cortex and extensive osteolysis with fracture (arrowhead).
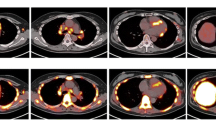
c Finger bone involvement seen on 18F-FDG PET
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Demaria, L., Borie, R., Benali, K. et al. 18F-FDG PET/CT in bone sarcoidosis: an observational study. Clin Rheumatol 39, 2727–2734 (2020). https://doi.org/10.1007/s10067-020-05022-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-020-05022-6