
Abstract
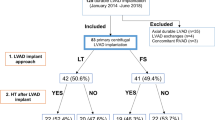
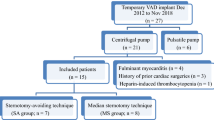
This is a single-center retrospective study to summarize clinical outcomes of patients requiring surgical continuous-flow left ventricular assist device (HeartMate II) exchange. The patients who underwent HeartMate II exchange were divided into two groups either via a subcostal approach (SC group) or a full sternotomy (FS group). The exclusion criteria of a subcostal approach for device exchange included the presence of outflow graft obstruction, and/or the need for concomitant cardiac procedures. Among 277 consecutive patients who underwent HeartMate II implantation from July 2008 to December 2015, 25 patients (9.0%) required device exchange (SC group; N = 13, FS group; N = 12). The SC group, compared to the FS group, had a shorter operative time (200.6 ± 31.4 min vs 534.2 ± 123.9 min; P < 0.001), shorter cardiopulmonary bypass time (33.1 ± 22.0 min vs 151.5 ± 53.1 min; P < 0.001), fewer blood transfusion (0.31 ± 0.48 units vs 4.67 ± 3.65 units; P = 0.002). The SC group had lower incidence of postoperative prolonged intubation (> 24 h) (7.7% vs 90.9%, P < 0.001), tracheostomy (0.0% vs 41.7%, P = 0.015), acute kidney injury requiring dialysis (0.0% vs 33.3%, P = 0.039). In-hospital mortality was 0.0% (0/13) in the SC group and 16.7% (2/12) in the FS group (P = 0.220). In conclusion, a subcostal approach was associated with shorter operative time, fewer blood transfusions, and less postoperative complications, compared to full sternotomy. A subcostal approach, if feasible, is preferred for HeartMate II device exchange.



Similar content being viewed by others

Change history
08 July 2020
In the original publication, the title of the article was published incorrectly.
References
Starling RC, Moazami N, Silevestry SC, Ewald G, Rogers JG, Milano CA, et al. Unexpected abrupt increase in left ventricular assist device thrombosis. N Eng J Med. 2014;370:33–40.
Xie A, Phan K, Yan TD. Durability of continuous-flow left ventricular assist devices: a systematic review. Ann Cardiothorac Surg. 2014;3:547–56.
Ota T, Yerebakan H, Akashi H, Takayama H, Uriel N, Colombo PC, et al. Continuous-flow left ventricular assist device exchange: clinical outcomes. J Heart Lung Transpl. 2014;33:65–70.
Soleimani B, Stephenson ER, Price LC, El-Banayosy A, Pae WE. Clinical experience with sternotomy versus subcostal approach for exchange of HeartMate II left ventricular assist device. Ann Thorac Surg. 2015;100:1577–80.
Levin AP, Uriel N, Takayama H, Mody KP, Ota T, Yuzefpolskaya M, et al. Device exchange in HeartMate II recipients: long-term outcomes and risk of thrombosis recurrence. ASAIO J. 2015;61:144–9.
Uriel N, Morrison KA, Garan AR, Kato TS, Yuzefpolskaya M, Latif F, et al. Development of a novel echocardiography ramp test for speed optimization and diagnosis of device thrombosis in continuous flow left ventricular assist devices: the Columbia Ramp Study. J Am Coll Cardiol. 2012;60:1764–75.
Nishimura T, Ota T, Takayama H, Naka Y. Subcostal to rib-cross incision for HeartMate II explantation: a case report. J Thorac Cardiovasc Surg. 2013;145:e16–7.
Levin AP, Saeed O, Willey JZ, Levin CJ, Fried JA, Patel SR, et al. Watchful waiting in continuous-flow left ventricular assist device patients with ongoing hemolysis is associated with an increased risk for cerebrovascular accident or death. Circ Heart Fail. 2016;9:e002896.
Stulak JM, Dunlay SM, Sharma S, Haglund NA, Davis MB, Cowger J, et al. Treatment of device thrombus in the HeartWare HVAD: Success and outcomes depend siginificantly on the initial treatment strategy. J Heart Lung Transpl. 2015;34:1535–41.
Raffa GM, D’Ancona G, Romano G, Falletta C, Sciacca S, Todaro C, et al. Should device replacement be the first choice strategy in continuous-flow left ventricle assist device thrombosis? Analysis of 9 events and results after endoventricular thrombolysis. Int J Cardiol. 2015;15:159–61.
Saeed D, Maxhera B, Albert A, Westenfeld R, Hoffmann T, Lichtenberg A. Conservative approaches for HeartWare ventricular assist device pump thrombosis may improve the outcome compared with immediate surgical approaches. Interact Cardiovasc Thorac Surg. 2016;23:90–5.
Oezpeker C, Zittermann A, Ensminger S, Kizner L, Koster A, Sayin A, et al. Systemic thrombolysis versus device exchange for pump thrombosis management: a single-center experience. ASAIO J. 2016;62:246–51.
Hammel D, Tjan DT, Scheld HH, Schmid C, Loick M, Deng MC. Successful treatment of a Novacor LVAD malfunction without repeat sternotomy. Thorac Cardiovasc Surg. 1998;46:154–6.
Ochiai Y, McCarthy PM, Smedira NG, Banbury MK, Navia JL, Feng J, et al. Predictors of severe right ventricular failure after implantable left ventricular assist device insertion: analysis of 245 patients. Circulation. 2002;106:198–202.
Furukawa K, Motomura T, Nose Y. Right ventricular failure after left ventricular assist device implantation: the need for an implantable right ventricular assist device. Artif Organs. 2005;29:369–77.
Chen JM, Levin HR, Rose EA, Addonizio LJ, Landry DW, Sistino JJ, et al. Experience with right ventricular assist devices for perioperative right sided circulatory failure. Ann Thorac Surg. 1996;61:305–10.
Pegg TJ, Selvanayagam JB, Karamitsos TD, Arnold RJ, Francis JM, Neubauer S, et al. Effects of off-pump versus on-pump coronary artery bypass grafting on early and late right ventricular function. Circulation. 2008;117:2202–10.
Kormos RL, Gasior TA, Kawai A, Pham SM, Murali S, Hattler BG, et al. Transplant candidate’s clinical status rather than right ventricular function defines need for univentricular versus biventricular support. J Thorac Cardiovasc Surg. 1996;111:773–82.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr Valluvan Jeevanandam discloses that he receives consultant fees from Abbott. Dr Nir Uriel discloses that he receives consultant fees and grant supports from Abbott, and Medtronic.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kitahara, H., Raikhelkar, J., Kim, G. et al. A subcostal approach is favorable compared to sternotomy for left ventricular assist device exchange field of research: artificial heart (clinical). J Artif Organs 22, 181–187 (2019). https://doi.org/10.1007/s10047-019-01102-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10047-019-01102-w