
Abstract
Objective
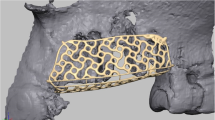
The study addresses the long-standing challenge of insufficient length in vascularized fibular flaps when reconstructing large mandibular defects that require dual-barrel grafts. Employing personalized 3D-printed osteotomy guides, the study aims to optimize fibular utilization and minimize the required graft length.
Material and methods
Two reconstruction methods for distal bone defects were compared: a fold-down (FD) group that employed a specialized osteotomy guide for folding down a triangular bone segment, and a traditional double-barrel (DB) group. Metrics for comparison included defect and graft lengths, as well as the graft-to-defect length ratio. Postoperative quality of life was assessed using the University of Washington Quality of Life questionnaire (UW-QoL).
Result
Both FD and DB groups achieved successful mandibular reconstruction. Despite larger defects in the FD group (117 ± 31.35 mm vs 84 ± 35.34 mm, p = 0.028), the used fibula length was not statistically longer in the FD group. The median ratio of graft-to-defect length was also lower in the FD group (1.327 vs 1.629, p = 0.024), suggesting that FD required only 82.47% of the graft length needed in the DB approach. Quality of life scores post-surgery were comparable between the groups.
Conclusion
Personalized 3D-printed osteotomy guides enhance fibula graft efficacy for reconstructing larger mandibular defects, necessitating shorter graft lengths while preserving postoperative quality of life.
Clinical relevance
This study confirms the utility of 3D printing technology as an effective and precise tool in orthopedic surgery, particularly for complex reconstructions like large mandibular defects. It suggests a viable alternative that could potentially revolutionize current practices in bone grafting.





Similar content being viewed by others


References
Hidalgo DA (1989) Fibula free flap: a new method of mandible reconstruction. Plast Reconstr Surg 84(1):71–79
Valentini V et al (2005) Surgical planning in reconstruction of mandibular defect with fibula free flap: 15 patients. J Craniofac Surg 16(4):601–607
Smolka K et al (2008) Fibula free flap reconstruction of the mandible in cancer patients: evaluation of a combined surgical and prosthodontic treatment concept. Oral Oncol 44(6):571–581
Chen J et al (2019) Functional mandibular reconstruction with double-barrel fibular flap and primary osseointegrated dental implants improve facial esthetic outcome. J Oral Maxillofac Surg 77(1):218–225
Horiuchi K et al (1995) Mandibular reconstruction using the double barrel fibular graft. Microsurgery 16(7):450–454
Muñoz Guerra MF et al (2001) Vascularized free fibular flap for mandibular reconstruction: a report of 26 cases. J Oral Maxillofac Surg 59(2):140–144
Shen Y et al (2013) Double-barrel vascularised fibula graft in mandibular reconstruction: a 10-year experience with an algorithm. J Plast Reconstr Aesthet Surg 66(3):364–371
He Y et al (2011) Double-barrel fibula vascularized free flap with dental rehabilitation for mandibular reconstruction. J Oral Maxillofac Surg 69(10):2663–2669
Zaretski A et al (2011) Biological reconstruction of bone defects: the role of the free fibula flap. J Child Orthop 5(4):241–249
Devireddy SK et al (2015) Evaluation of non-vascular fibula graft for mandibular reconstruction. J Maxillofac Oral Surg 14(2):299–307
Lu T et al (2020) Recent advance in patient-specific 3D printing templates in mandibular reconstruction. J Mech Behav Biomed Mater 106:103725
Li Y et al (2020) Virtual surgical planning for successful second-stage mandibular defect reconstruction using vascularized iliac crest bone flap: a valid and reliable method. Ann Plast Surg 84(2):183–187
Zho M et al (2019) Comparison of complicated and simple guiding templates in mandibular reconstruction using vascularized iliac crest flap. Biomed Res Int 2019:7496538
Wu TF et al (2019) Matching locating holes in multiple plates to record bone position for accurate reconstruction after segmental mandibulectomy. Int J Oral Maxillofac Surg 48(12):1516–1519
Hsing C et al (2011) Comparison between free flap and pectoralis major pedicled flap for reconstruction in oral cavity cancer patients–a quality of life analysis. Oral Oncol 47(6):522–527
Weymuller E et al (2001) Analysis of the performance characteristics of the University of Washington Quality of Life instrument and its modification (UW-QOL-R). Arch Otolaryngol-Head Neck Surg 127(5):489–93
Rogers S et al (2002) The addition of mood and anxiety domains to the University of Washington quality of life scale. Head Neck 24(6):521–529
Schlieve T et al (2015) Is immediate reconstruction of the mandible with nonvascularized bone graft following resection of benign pathology a viable treatment option? J Oral maxillofac Surg: Off J Am Assoc Oral Maxillofac Surg 73(3):541–549
Akinbami B (2016) Reconstruction of continuity defects of the mandible with non-vascularized bone grafts. Systematic literature review. Craniomaxillofacial Trauma Reconstr 9(3):195–205
Nandra B et al (2017) Free bone grafts for mandibular reconstruction in patients who have not received radiotherapy: the 6-cm rule-myth or reality? Craniomaxillofac Trauma Reconstr 10(2):117–122
Shin JY et al (2022) Association between non-vascularised bone graft failure and compartment of the defect in mandibular reconstruction: a systematic review and meta-analysis. Br J Oral Maxillofac Surg 60(2):128–133
Pogrel M et al (1997) A comparison of vascularized and nonvascularized bone grafts for reconstruction of mandibular continuity defects. J Oral Maxillofac Surg: Off J Am Assoc Oral Maxillofac Surg 55(11):1200–1206
Foster R et al (1999) Vascularized bone flaps versus nonvascularized bone grafts for mandibular reconstruction: an outcome analysis of primary bony union and endosseous implant success. Head Neck 21(1):66–71
Funding
This study was supported by grants from the Health Commission of Hubei Province scientific research project (No. WJ2021M179 to Tianfu Wu and No. WJ2021M175 to Bing Liu and No. WJ2023M122 to Lin Dai) and Translational Medicine and Interdisciplinary Research Joint Fund of Zhongnan Hospital of Wuhan University (ZNJC202242) to Bo Cheng.
Author information
Authors and Affiliations
Contributions
Lei Jiang and Hao Lin drafted the manuscript and data analysis. Zhixiang Ge, Zhe Shao prepared the guide and 3D-printed osteotomy guides. Dai Lin, Tianfu Wu, Bo Cheng and Bing Liu performed all the surgeries and provided constructive suggestions to the manuscipt.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Regional Ethical Review Board of the School & Hospital of Stomatology of Wuhan University and followed the Declaration of Helsinki [2018]/B(29). Written informed consent was obtained from all patients before surgery.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Lei Jiang and Hao Lin contribute equally to this work.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Jiang, L., Lin, H., Shao, Z. et al. Efficacy of personalized 3D-printed osteotomy guide in maximizing fibular utilization and minimizing graft length for reconstruction of large mandibular defect. Clin Oral Invest 28, 125 (2024). https://doi.org/10.1007/s00784-024-05519-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00784-024-05519-3