
Abstract
Objectives
Defects after ablative tongue cancer surgery can be reconstructed by split-thickness skin grafts or free microvascular flaps. The different surgical options may influence costs, reimbursement, and therefore possible profits. Our goal was to analyze the development of these parameters for different procedures in head and neck reconstruction in Germany over the last decade.
Materials and methods
After tumor resection and neck dissection of tongue cancer, three different scenarios were chosen to calculate costs, reimbursement, length of stay (LoS), and profits. Two options considered were reconstruction by split-thickness skin graft with (option Ia) and without (option Ib) tracheotomy. In addition, we analyzed microvascular reconstruction with radial forearm flap (option II). Furthermore, unsatisfactory results after options Ia and Ib may make secondary tongue plastic with split-thickness skin grafting necessary (option I+). The calculations were performed considering the German Diagnosis Related Group (DRG) system and compared to the specific DRG cost data of 250 German reference hospitals.
Results
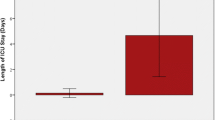
The overall average length of stay (aLoS) declined from 16.7 to 12.8 days with a reduction in every option. Until 2011, all options showed similar accumulated DRG reimbursement. From 2012 onwards, earnings almost doubled for option II due to changes in the DRG allocation. As was expected, the highest costs were observed in option II. Profits (reimbursement minus costs) were also highest for option II (mean 2052 €, maximum 3630 Euros in 2015) followed by options Ia (765 €) and Ib/I+ (681 €). Average profits over time would be 17 to 19% higher if adjusted for inflation.
Conclusions
We showed the development of the DRG allocation of two commonly used methods of reconstruction after ablative tongue cancer surgery and the associated LoS, reimbursement, costs, and profits. As expected, the highest values were found for microvascular reconstruction. Microvascular reconstruction may also be the primary choice of treatment from a medical point of view. However, prolonged operation times, intensive care, and hospital stay in connection with complex microvascular operations can easily turn profits into losses as opposed to the results of simple, reliable, and fast split-thickness skin grafting. The inflation rate influences profits in reimbursement systems where costs are based on a previous period of time.
Clinical relevance
Surgeons find themselves daily in an area of conflict between economic interests and medical decision-making. Due to its multidimensional aspects, the choice of the reconstructive technique should be primarily based on the best medical care for the patient. But there should also be awareness of the economic risk of all three surgical procedures.




Similar content being viewed by others


References
Campana JP, Arlen D, Meyers AD (2006) The surgical management of oral cancer. Otolaryngol Clin N Am 39:331–348
Brown L, Rieger JM, Harris J, Seikaly H (2010) A longitudinal study of functional outcomes after surgical resection and microvascular reconstruction for oral cancer: tongue mobility and swallowing function. J Oral Maxillofac Surg 68:2690–2700
Smith GI, Yeo D, Clark J, Choy ET, Gao K, Oates J, O’Brien CJ (2006) Measures of health-related quality of life and functional status in survivors of oral cavity cancer who have had functional defects reconstructed with radial forearm free flaps. Br J Oral Maxillofac Surg 44:187–192
Rhemrev R, Rakhorst HA, Zuidam JM, Mureau MAM, Hovius SER, Hofer SOP (2007) Long-term functional outcome and satisfaction after forearm free flap reconstructions of intraoral malignancy resections. J Plast Reconstr Aesthet Surg 60:588–592
Klein M (2012) Operationen des Gesichts und der Kopfhaut. In: Hausamen JE, Machtens E, Reuther J, Eufinger H, Kübler A, Schliephake H (eds) Mund-, Kiefer- und Gesichtschirurgie, 4th edn. Springer, Berlin, Heidelberg, pp 4467–4468
Harashina T, Fujino T, Aoyagi F (1976) Reconstruction of the oral cavity with a free flap. Plast Reconstr Surg 58:412
Panje WR, Bardach J, Krause CJ (1976) Reconstruction of the oral cavity with a free flap. Plast Reconstr Surg 58:415
Yang G, Chen B, Gao Y et al (1981) Forearm free skin transplantation. Nat Med J China 61:139–142
Song R, Gao Y, Song Y et al (1982) The forearm flap. Clin Plast Surg 9:21–26
Wolff KD (2011) Radial forearm flap. In: Wolff KD, Hoelzle F (eds) Raising of microvascular flaps. A systematic approach, 1st edn. Springer, Berlin, pp 1–20
Jones NF, Jarrahy R, Song JI, Kaufman MR, Markowitz B (2007) Postoperative medical complications—not microsurgical complications—negatively influence the morbidity, mortality, and true costs after microsurgical reconstruction for head and neck cancer. Plast Reconstr Surg 119:1053–2060
Chien CY, Hwang CF, Chuang HC, Jeng SF, Su CY (2005) Comparison of radial forearm free flap, pedicled buccal fat flap and split-thickness skin graft in reconstruction of buccal mucosal defect. Oral Oncol 41:694–697
Bozec A, Poissonnet G, Chamorey E, Casanova C, Laout C, Vallicioni J, Demard F, Peyrade F, Follana P, Bensadoun RJ, Benezery K, Thariat J, Marcy PY, Sudaka A, Weber P, Dassonville O (2009) Quality of life after oral and oropharyngeal reconstruction with a radial forearm free flap: prospective study. J Otolaryngo Head Neck Surg 38:401–408
Ewers R, Hoffmeister B (1988) Reconstruction of the mandibular denture bearing area and freeing of the tongue after tumor surgery. J Oral Maxillofac Surg 46:272–275
Institut für das Entgeltsystem im Krankenhaus. G-DRG-System (2016) http://www.g-drg.de/cms. Accessed April 3, 2016
GKV-Spitzenverband. G-DRG-System 2016. http://www.gkv-spitzenverband.de/KH_DRG_System_G_DRG_2016.gkvnet. Accessed April 6, 2016 15
ID Information und Dokumentation im Gesundheitswesen GmbH & Co KGaA, Berlin/Germany (2016). http://www.id-berlin.de/de/products. Accessed May 22, 2016
Wissenschaftliches Institut der Allgemeinen Ortskrankenkassen: Z-Bax – Preisindex der Zahlbasisfallwerte (2016) https://www.wido.de/fileadmin/wido/downloads/pdf_krankenhaus/Z-Bax/wido_kra_zbax_20171027.pdf. Accessed November 8, 2017
Statistisches Bundesamt Deutschland: Verbraucherpreisindex (2016). http://www.destatis.de/jetspeed/portal/cms/Sites/destatis/Internet/DE/Presse/abisz/VPI.psml. Accessed Februar 22, 2016
McConnel FMS, Teichgraeber JF, Adler RK (1987) A comparison of three methods of oral reconstruction. Arch Otolaryngol Head Neck Surg 113:496–500
Alvi A, Myers EN (1996) Skin graft reconstruction of the composite resection defect. Head Neck 18:538–544
Schramm VL, Johnson JT, Myers EN (1983) Skin grafts and flap in oral cavity reconstruction. Arch Otolaryngol 109:175–177
Brown JS, Magennis P, Rogers SN, Cawood JI, Howell R, Vaughan ED (2006) Trend in head neck microvascular reconstructive surgery in Liverpool (1992-2001). Br J Maxillofac Surg 44:364–370
Kroll SS, Evans GR, Goldberg D et al (1997) A comparison of resource costs for head and neck reconstruction with free and pectoralis major flaps. Plast Reconstr Surg 99:1282–1286
McCrory AL, Magnuson JS (2002) Free tissue transfer versus pedicled flap in head and neck reconstruction. Laryngoscope 112:2161–2165
Smeele LE, Goldstein D, Tsai V et al (2006) Morbidity and cost differences between free flap reconstruction in oral and oropharyngeal cancer: matched control study. J Otolaryngol 35:102–107
Tsue TT, Desyatnikova SS, Deleyiannis FW et al (1997) Comparison and function in reconstruction of the posterior oral cavity and oropharynx. Free vs pedicled soft tissue transfer. Arch Otolaryngol Head Neck Surg 123:731–737
De Bree R, Reith R, Quak JJ et al (2007) Free radial forearm flap versus pectoralis mayor myocutaneous flap reconstruction of oral and oropharyngeal defects: a cost analysis. Clin Otolaryngol 32:275–282
Deganello A, Gitti G, Parrinello G et al. (2013) Cost analysis in oral cavity and oropharyngeal reconstruction with microvascular and pedicled flaps 33:380–387
Twieg M, Reich W, Dempf R, Eckert AW (2014) Renaissance of pedicled flaps in oral and maxillofacial surgery. Chirurg 85:529–536
Chalian AA, Kagan SH, Goldberg AN, Gottschalk A, Dakunchak A, Weinstein GS, Weber RS (2002) Arch Otolaryngol Head Neck 128:892–896
Schwenzer T, Jaehne J (2012) Patientenauswahl in Krankenhaeusern der Maximalversorgung auf Basis oekonomischer Daten. Chirurg 83:259–267
Harrison WL, Bhattacharyya N (2011) Contemporary assessment of medical morbidity and mortality in head and neck surgery. Otolaryngol Head Neck Surg 146:385–389
Ryan MW, Hochman M (2000) Length of stay after free flap reconstruction of head and neck. Laryngoscope 110:210–216
Petruzzelli GJ, Brockenbrough JM, Vandevender D, Creech SD (2002) The influence of reconstructive modality on cost of care in head and neck oncologic surgery. Arch Otolaryngol Head Neck Surg 128:1377–1380
Deutsche Krebsgesellschaft Kennzahlenauswertung 2016 Jahresbericht der zertifizierten Kopf-Hals-Tumor-Zentren (Auditjahr 2017). https://www.krebsgesellschaft.de/jahresberichte.html
Talesnik A, Markowitz B, Calcaterra T, Ahn C, Shaw W (1996) Cost and outcome of osteocutaneous free-tissue transfer versus pedicled soft-tissue reconstruction for composite mandibular defects. Plast Reconstr Surg 97:1167–1178
Rosenthal E, Carroll W, Dobbs M, Magnuson JS, Wax M, Peters G (2004) Simplifying head and neck microvascular reconstruction. Head Neck 26:930–936
Acknowledgements
The authors like to express their sincere thanks to Dr. Cintia S. De Paiva, MD, Ocular Surface Center, Department of Opthalmology, Baylor College of Medicine, Houston, Texas and Dr. Martin Widmann, MD, Departement of Oral and Maxillofacial Surgery, University Hospital Tuebingen, Germany, for their proofreading of the manuscript and critical remarks.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Hoefert, S., Lotter, O. Change in reimbursement and costs in German oncological head and neck surgery over the last decade: ablative tongue cancer surgery and reconstruction with split-thickness skin graft vs. microvascular radial forearm flap. Clin Oral Invest 22, 1741–1750 (2018). https://doi.org/10.1007/s00784-017-2269-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-017-2269-x