
Abstract
Objectives
This study aims to evaluate periodontal microbiological differences between systemically healthy nonsmoker males taking anabolic androgenic steroids (AASs) and non-AAS users and to find associations between disease severity and AAS use.
Methods
Ninety-two men practicing bodybuilding were included in the study. They were divided into AAS users and a matched control nonuser group and subgrouped based on their most severe periodontal condition. Pooled subgingival samples from each individual were cultured to evaluate specific periodontopathogen infection.
Results
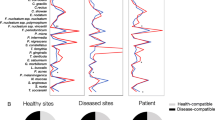
AAS users had significantly higher prevalence of severe periodontitis. AAS users had greater gingival inflammation and clinical attachment loss of ≥3 mm than nonusers (odds ratio (OR) = 2.4; p = 0.09; 95 % confidence interval (CI) 0.8–6.4). AAS users were 4.9 times more likely to be infected with Prevotella intermedia than AAS nonusers (OR = 4.9; p = 0.003; 95 % CI 1.6–14.7). The OR of presenting subgingival Aggregatibacter actinomycetemcomitans was 8.2 times higher in AAS users (OR = 8.2; p = 0.03; 95 % CI 0.9–70.8). AAS users were 5.6 times more likely to present subgingival Candida spp. than nonusers (OR = 5.6; p = 0.02; 95 % CI 1.1–27.1). AAS users were 14.8 times more likely to present subgingival Candida parapsilosis than nonusers (OR = 14.8; p < 0.0001; 95 % CI 3.1–69.2). The likelihood of AAS users presenting subgingival Candida tropicalis was 4.3 times higher than nonusers (OR = 4.3; p = 0.03; 95 % CI 1.1–16.9). A. actinomycetemcomitans was mostly isolated in individuals with severe periodontitis and was associated with subgingival Porphyromonas gingivalis, P. intermedia, and Candida spp.
Conclusions
AAS use may increase the risk for severe periodontitis and may cause a subgingival selection of certain Candida species. Specific periodontopathogens, such as Candida dubliniensis and Candida albicans, seem to be negatively affected by AAS use. The higher risk for disease progression in AAS users may be explained by the significantly higher proportions of A. actinomycetemcomitans, P. gingivalis, P. intermedia, and Candida species as compared to controls.
Clinical significance
Data on the influence of AAS on subgingival periodontopathogens and disease progression are scarce. Higher proportions of specific periodontopathogens are plausible in AAS users. AAS users had a higher prevalence of severe periodontitis, gingival inflammation, and clinical attachment loss. Men taking AAS are at greater risk of periodontitis and specific periodontopathogen infection.
Similar content being viewed by others

References
Orr R, Fiatarone Singh M (2004) The anabolic androgenic steroid oxandrolone in the treatment of wasting and catabolic disorders: review of efficacy and safety. Drugs 64:725–750
Basaria S, Wahlstrom JT, Dobs AS (2001) Clinical review 138: anabolic-androgenic steroid therapy in the treatment of chronic diseases. J Clin Endocrinol Metab 86:5108–5117
Maior AS, Simao R, de Salles BF, Alexander JL, Rhea M, Nascimento JH (2010) Acute cardiovascular response in anabolic androgenic steroid users performing maximal treadmill exercise testing. J Strength Cond Res 24:1688–1695
Arvary D, Pope HG Jr (2000) Anabolic-androgenic steroids as a gateway to opioid dependence. N Engl J Med 342:1532
Ip EJ, Barnett MJ, Tenerowicz MJ, Perry PJ (2011) The Anabolic 500 survey: characteristics of male users versus nonusers of anabolic-androgenic steroids for strength training. Pharmacotherapy 31:757–766
Kanayama G, Hudson JI, Pope HG Jr (2009) Features of men with anabolic-androgenic steroid dependence: a comparison with nondependent AAS users and with AAS nonusers. Drug Alcohol Depend 102:130–137
Sader MA, Griffiths KA, McCredie RJ, Handelsman DJ, Celermajer DS (2001) Androgenic anabolic steroids and arterial structure and function in male bodybuilders. J Am Coll Cardiol 37:224–230
Graham MR, Davies B, Grace FM, Kicman A, Baker JS (2008) Anabolic steroid use: patterns of use and detection of doping. Sports Med 38:505–525
Sjoqvist F, Garle M, Rane A (2008) Use of doping agents, particularly anabolic steroids, in sports and society. Lancet 371:1872–1882
Kasasa SC, Soory M (1996) The synthesis of 5-alpha-dihydrotestosterone from androgens by human gingival tissues and fibroblasts in culture in response to TGF-beta and PDGF. J Periodontal Res 31:313–322
Brusca MI, Rosa A, Albaina O, Moragues MD, Verdugo F, Ponton J (2010) The impact of oral contraceptives on women's periodontal health and the subgingival occurrence of aggressive periodontopathogens and Candida species. J Periodontol 81:1010–1018
Ozcelik O, Haytac MC, Seydaoglu G (2006) The effects of anabolic androgenic steroid abuse on gingival tissues. J Periodontol 77:1104–1109
Coletta RD, Reynolds MA, Martelli-Junior H, Graner E, Almeida OP, Sauk JJ (2002) Testosterone stimulates proliferation and inhibits interleukin-6 production of normal and hereditary gingival fibromatosis fibroblasts. Oral Microbiol Immunol 17:186–192
Famili P, Cauley JA, Greenspan SL (2007) The effect of androgen deprivation therapy on periodontal disease in men with prostate cancer. J Urol 177:921–924
Soory M (2000) Targets for steroid hormone mediated actions of periodontal pathogens, cytokines and therapeutic agents: some implications on tissue turnover in the periodontium. Curr Drug Targets 1:309–325
Soory M, Tilakaratne A (2003) Anabolic potential of fibroblasts from chronically inflamed gingivae grown in a hyperglycemic culture medium in the presence or absence of insulin and nicotine. J Periodontol 74:1771–1777
Engeland CG, Sabzehei B, Marucha PT (2009) Sex hormones and mucosal wound healing. Brain Behav Immun 23:629–635
Silness J, Loe H (1964) Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand 22:121–135
Loe H, Silness J (1963) Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand 21:533–551
Dahlen G, Pipattanagovit P, Rosling B, Moller AJ (1993) A comparison of two transport media for saliva and subgingival samples. Oral Microbiol Immunol 8:375–382
Sahand IH, Moragues MD, Eraso E, Villar-Vidal M, Quindos G, Ponton J (2005) Supplementation of CHROMagar Candida medium with Pal's medium for rapid identification of Candida dubliniensis. J Clin Microbiol 43:5768–5770
Brena S, Rubio Mdel C, Salesa R et al (2004) Genotypes of Candida dubliniensis in clinical isolates. Rev Iberoam Micol 21:20–23
Sahand IH, Moragues MD, Robert R, Quindos G, Ponton J (2006) Evaluation of Bichro-Dubli Fumouze to distinguish Candida dubliniensis from Candida albicans. Diagn Microbiol Infect Dis 55:165–167
Bikandi J, Millan RS, Moragues MD et al (1998) Rapid identification of Candida dubliniensis by indirect immunofluorescence based on differential localization of antigens on C. dubliniensis blastospores and Candida albicans germ tubes. J Clin Microbiol 36:2428–2433
Sooriyamoorthy M, Gower DB (1989) Hormonal influences on gingival tissue: relationship to periodontal disease. J Clin Periodontol 16:201–208
Mariotti A (1994) Sex steroid hormones and cell dynamics in the periodontium. Crit Rev Oral Biol Med 5:27–53
Gilliver SC (2010) Sex steroids as inflammatory regulators. J Steroid Biochem Mol Biol 120:105–115
Steffens JP, Coimbra LS, Ramalho-Lucas PD, Rossa C Jr, Spolidorio LC (2012) The effect of supra- and subphysiologic testosterone levels on ligature-induced bone loss in rats—a radiographic and histologic pilot study. J Periodontol 83:1432–1439
Daltaban O, Saygun I, Bolu E (2006) Periodontal status in men with hypergonadotropic hypogonadism: effects of testosterone deficiency. J Periodontol 77:1179–1183
Orwoll ES, Chan BK, Lambert LC, Marshall LM, Lewis C, Phipps KR (2009) Sex steroids, periodontal health, and tooth loss in older men. J Dent Res 88:704–708
Jewtuchowicz VM, Mujica MT, Brusca MI et al (2008) Phenotypic and genotypic identification of Candida dubliniensis from subgingival sites in immunocompetent subjects in Argentina. Oral Microbiol Immunol 23:505–509
Jabra-Rizk MA, Ferreira SM, Sabet M, Falkler WA, Merz WG, Meiller TF (2001) Recovery of Candida dubliniensis and other yeasts from human immunodeficiency virus-associated periodontal lesions. J Clin Microbiol 39:4520–4522
Portela MB, Souza IP, Costa EM, Hagler AN, Soares RM, Santos AL (2004) Differential recovery of Candida species from subgingival sites in human immunodeficiency virus-positive and healthy children from Rio de Janeiro, Brazil. J Clin Microbiol 42:5925–5927
Urzua B, Hermosilla G, Gamonal J et al (2008) Yeast diversity in the oral microbiota of subjects with periodontitis: Candida albicans and Candida dubliniensis colonize the periodontal pockets. Med Mycol 46:783–793
Jarvensivu A, Hietanen J, Rautemaa R, Sorsa T, Richardson M (2004) Candida yeasts in chronic periodontitis tissues and subgingival microbial biofilms in vivo. Oral Dis 10:106–112
Slots J, Rams TE, Listgarten MA (1988) Yeasts, enteric rods and pseudomonads in the subgingival flora of severe adult periodontitis. Oral Microbiol Immunol 3:47–52
Acknowledgments
This work has been partially financed with grants IT-264-07 from the Department of Education, Universities and Research, Basque Government, and UFI11/25 from the University of Basque Country UPV/EHU (to MDM). We would like to thank Professor José Pontón, Microbiology, Immunology and Parasitology Department, University of Basque Country, Leioa, Spain, for his past direction and guidance.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brusca, M.I., Verdugo, F., Amighini, C. et al. Anabolic steroids affect human periodontal health and microbiota. Clin Oral Invest 18, 1579–1586 (2014). https://doi.org/10.1007/s00784-013-1126-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-013-1126-9