
Abstract
Background
The presigmoid approach classically includes the ligature and section of the superior petrosal sinus to get a wider visibility window to the antero-lateral brainstem surface. In some cases, the separation of this venous structure should not be performed.
Method
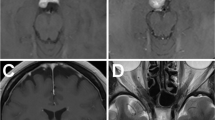
We present our experience getting safely to a pontine cavernous malformation through a conventional mastoidectomy presigmoid approach preserving an ingurgitated superior petrosal sinus because the association with an abnormal venous drainage of the brainstem.
Conclusions
When sectioning the superior petrosal sinus in classical presigmoid approaches is contraindicated, its preservation could also offer good surgical corridors to get to small-medium anterior and lateral brainstem cavernous malformations.






Similar content being viewed by others


Abbreviations
- SPS:
-
Superior petrosal sinus
- AVD:
-
Abnormal venous drainage
- CN:
-
Cranial nerves
- TS:
-
Transverse sinus
- SS:
-
Sigmoid sinus
- SCC:
-
Semicircular canals
- LSCC:
-
Lateral semicircular canal
- PSCC:
-
Posterior semicircular canal
- TT:
-
Trautmann triangle
References
Almefty KK, Al-Mefty O (2021) Petrosal approach with preservation of the superior petrosal sinus (the graceful petrosal) for resection of giant trigeminal schwannoma: 2-dimensional operative video. Oper Neurosurg (Hagerstown) 20(5):E342–E343. https://doi.org/10.1093/ons/opaa427
Al-Mefty O, Fox JL, Smith RR (1988) Petrosal approach for petroclival meningiomas. Neurosurgery 22:510–517. https://doi.org/10.1227/00006123-198803000-00010
Friedman RA, Brackmann DE, van Loveren HR, Hitselberger WE (1997) Management of the contracted mastoid in the translabyrinthine removal of acoustic neuroma. Arch Otolaryngol Head Neck Surg 123(3):342–344. https://doi.org/10.1001/archotol.1997.01900030128016
Hakuba A, Nishimura S, Jang BJ (1988) A combined retroauricular and preaurical transpetrosal-transtentorial approach to the clivus meningiomas. Surg Neurol 30:108–116. https://doi.org/10.1016/0090-3019(88)90095-x
Hauck EF, Barnett SL, White JA, Samson D (2010) The presigmoid approach to anterolateral pontine cavernomas. Clinical article J Neurosurg 113(4):701–708. https://doi.org/10.3171/2010.1.JNS08413
Kulwin CG, Payner TD, Nelson RF, Ackerman LL, Fulkerson DH (2018) Pediatric pontine cavernous malformations: the presigmoid, posterior petrosal approach. Oper Neurosurg (Hagerstown) 15(5):522–529. https://doi.org/10.1093/ons/opy007
Oiwa Y, Nakai K, Masaki Y et al (2002) Presigmoid approach for cavernous angioma in the pons—technical note. Neurol Med Chir (Tokyo) 42(2):91–98. https://doi.org/10.2176/nmc.42.91
Thomas N, Maratos E, Barazi S (2019) Combined supra- and infra-tentorial retro-labyrinthine pre-sigmoid approach. Curr Otorhinolaryngol Rep 7:195–199. https://doi.org/10.1007/s40136-019-00226-0
Troude L, Baucher G, Lavieille JP, Roche PH (2021) The presigmoid retrolabyrinthine approach: technical note. Neurochirurgie 67(5):503–507. https://doi.org/10.1016/j.neuchi.2021.01.008
Yeh YC, Wei KC, Chen KT (2020) Transmastoid presigmoid retrolabyrinthine approach for removal of pontine cavernous malformation: how I do it. Acta Neurochir (Wien) 162(5):1131–1135. https://doi.org/10.1007/s00701-020-04263-3
Acknowledgements
We would like to thank to Dr. Maria J Mayorga, our pediatric anesthesiologist for all the support, to Dr. Ariel Kaen and Dr. Eugenio Cárdenas, including the rest of our Neurological Surgery department at Virgen del Rocío University Hospital, for all the usual support in research and investigation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Not applicable.
Consent to participate
The patient and her parents have consented to the submission of this article to the journal.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
Preoperative study by contrast MRI and tractography. Evaluation of compromised neurovascular structures, major neuronal pathways and AVDs presence even with angiography, is crucial.
Preservation of superior petrosal sinus! When indicated, this is a good and acceptable limited way to get to small and medium anterior and lateral brainstem lesions.
Prevent extensive venous infarctions. Preservation of AVDs is important to minimize risk and comorbidities.
Precaution! When IONM alerts of neurological impairment during surgery, remember resting, irrigation, and corticoids bolus rescue doses.
Bony structures and venous sinuses variation assessment. It is mandatory to evaluate and predict possible problems with the Trautmann triangle delimitation and aeration of mastoid.
Check and preserve the semicircular posterior and lateral canals. They will be our anterior TT limits for drilling.
Get indocyanine green. When dealing with non-exophytic lesions, intraoperative fluorescein could be helpful to select the better and safer point to enter the brainstem.
Neurological surveillance. Intraoperative neurophysiological monitoring (INMO) is always suitable in this type of surgeries.
Add corticosteroids postoperatively. Short therapies are related to neurological improvement after surgery.
Evaluate the indication of surgery. Neurological impairment and rebleeding are the first conditions to indicate surgical treatment.
This article is part of the Topical Collection on Neurosurgical technique evaluation
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 48666 KB)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Butrón-Díaz, C., Romero-López, C., Rivero-Garvia, M. et al. Presigmoid approach preserving the superior petrosal sinus in a pontine cavernous malformation associated to abnormal venous drainage of the brainstem: how I do it. Acta Neurochir 165, 1233–1240 (2023). https://doi.org/10.1007/s00701-022-05407-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-022-05407-3