
Abstract
Background
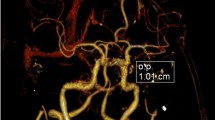
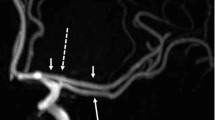
Moyamoya disease (MMD) is a chronic progressive disease leading to recurrent stroke due to occlusion of the terminal internal carotid arteries. Surgical revascularization for symptomatic MMD is an effective treatment for preventing further stroke. However, direct revascularization of advanced MMD remains challenging due to small caliber of the recipient vessel and perforators.
Methods
We introduce our technique of superficial temporal artery (STA) to middle cerebral artery (MCA) bypass with figures and video to illustrate the procedure.
Conclusion
Surgical nuances of STA to MCA anastomosis will help cerebrovascular neurosurgeons to master low-flow bypass for MMD.




Similar content being viewed by others
References
Chen TH, Chen CH, Shyu JF, Wu CW, Lui WY, Liu JC (1999) Distribution of the superficial temporary artery in the Chinese adult. Plast Reconstr Surg 104:1276–1279
Guzman R, Steinberg GK (2010) Direct bypass techniques for the treatment of pediatric moyamoya disease. Neurosurg Clin N Am 21:565–573
Ishii K, Fujiki M, Kobayashi H (2008) Invited article: surgical management of moyamoya disease. Turk Neurosurg 18:107–113
Kuroda S, Houkin K (2012) Bypass surgery for moyamoya disease: concept and essence of surgical techniques. Neurol Med Chir (Tokyo) 52:287–294
Rutledge C, Raper DMS, Abla AA (2020) How I do it: superficial temporal artery-middle cerebral artery bypass for flow augmentation and replacement. Acta Neurochir (Wien) 162:1847–1851
Wanebo JE, Zabramski JM, Spetzler RF (2004) Superficial temporal artery-to-middle cerebral artery bypass grafting for cerebral revascularization. Neurosurgery 55:395–398
Xu B, Song DL, Mao Y, Gu YX, Xu H, Liao YJ, Liu CH, Zhou LF (2012) Superficial temporal artery-middle cerebral artery bypass combined with encephalo-duro-myo-synangiosis in treating moyamoya disease: surgical techniques, indications and midterm follow-up results. Chin Med J (Engl) 125:4398–4405
Yasargil MG, Yonekawa Y (1977) Results of microsurgical extra-intracranial arterial bypass in the treatment of cerebral ischemia. Neurosurgery 1:22–24
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Approval was obtained from the ethics committee of Huashan Hospital, Fudan University. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Informed consent was obtained from individual participant included in the study.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
1. Perioperative blood pressure monitoring is important.
2. The middle meningeal artery should be preserved during craniotomy.
3. Dissecting the parietal branch of the STA from the scalp flap is a safe and rapid way.
4. Periadventitial tissues are dissected from the STA using sharp dissection.
5. Two slightly curved miniclips are used to temporarily occlude the recipient artery without sacrificing any perforators.
6. The bypass is initiated at the toe stitch so as to appropriately match donor with recipient.
7. Square knot is carefully made without any kinking of the suture.
8. Interrupted sutures are performed on each side of the arteriotomy.
9. Grasping the intima should be avoided during traction and countertraction on the vessels being sutured.
10. Bypass patency is confirmed with intraoperative ICG angiography.
This article is part of the Topical Collection on Vascular Neurosurgery—Ischemia
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 74839 KB) Video 1: STA-MCA bypass for MMD
Rights and permissions
About this article

Cite this article
Liao, Y., Xu, F. & Xu, B. How I do it: superficial temporal artery to middle cerebral artery bypass for moyamoya disease. Acta Neurochir 164, 1855–1859 (2022). https://doi.org/10.1007/s00701-022-05255-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-022-05255-1