
Abstract
Background
The petrous apex is one of the most challenging areas of the skull base to access.
Method
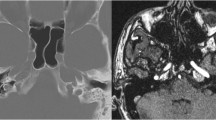
We present a case of residual petrous apex chordoma posterolateral to the paraclival segment of the internal carotid artery (ICA) resected with combined endoscopic endonasal and contralateral transmaxillary (CTM) approaches, without lateralization of the ICA.
Conclusion
This case demonstrates the value of the CTM corridor in resecting petrous apex lesions that are posterolateral to the paraclival segment of the ICA.






Similar content being viewed by others


References
Eytan DF, Kshettry VR, Sindwani R, Woodard TD, Recinos PF (2014) Surgical outcomes after endoscopic management of cholesterol granulomas of the petrous apex: a systematic review. Neurosurg Focus 37:E14. https://doi.org/10.3171/2014.7.FOCUS14344
Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R (2005) Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 19:E6.:190106 [pii]
Lavigne P, Wang EW, Fernandez-Miranda JC (2019) Supratotal resection of residual clival chordoma with combined endoscopic endonasal and contralateral transmaxillary approaches: 2-dimensional operative video. Oper Neurosurg 16:E88–E89. https://doi.org/10.1093/ons/opy220
Lawrence JD, Marsh R, Turner MT (2021) Contralateral transmaxillary approach for resection of chondrosarcoma of the petrous apex: a case report. Ear Nose Throat J:145561320982161. https://doi.org/10.1177/0145561320982161
Pamias-Portalatin E, Mahato D, Rincon-Torroella J, Vivas-Buitrago T, Quinones-Hinojosa A, Boahene KO (2018) Endoscope-assisted contralateral transmaxillary approach to the clivus and the hypoglossal canal: technical case report. J Neurosurg:1–7. https://doi.org/10.3171/2018.1.JNS171972
Patel CR, Wang EW, Fernandez-Miranda JC, Gardner PA, Snyderman CH (2018) Contralateral transmaxillary corridor: an augmented endoscopic approach to the petrous apex. J Neurosurg 129:211–219. https://doi.org/10.3171/2017.4.JNS162483
Razek AA, Huang BY (2012) Lesions of the petrous apex: classification and findings at CT and MR imaging. Radiographics 32:151–173. https://doi.org/10.1148/rg.32110575832/1/151[pii]
Snyderman CH, Gardner PA, Wang EW, Fernandez-Miranda JC, Valappil B (2021) Experience with the endoscopic contralateral transmaxillary approach to the petroclival skull base. Laryngoscope 131:294–298. https://doi.org/10.1002/lary.28740
Wang WH, Lan MY, Snyderman CH, Gardner PA (2021) Combined endoscopic endonasal and contralateral transmaxillary approach for petrous cholesteatoma: 2-dimensional operative video. Oper Neurosurg 20:E434–E435. https://doi.org/10.1093/ons/opab004
Zanation AM, Snyderman CH, Carrau RL, Gardner PA, Prevedello DM, Kassam AB (2009) Endoscopic endonasal surgery for petrous apex lesions. Laryngoscope 119:19–25. https://doi.org/10.1002/lary.20027
Funding
This study was sponsored by CAMS Innovation Fund for Medical Sciences (CIFMS, 2019-I2M-5–008)。
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
Not required.
Consent for publication
It represents a video of a surgical case. The patient approved for this publication.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
1. Chondromatous tumors, including chordomas and chondrosarcomas, are the most common in the petrous apex.
2. The epidural anterior petrosectomy (Kawase approach) directly accesses the petrous apex lesions from the lateral aspect. Although it still carries a minor potential risk of brain edema and seizure, it might be the number one strategy for many skull base neurosurgeons.
3. The routine endoscopic endonasal approach (EEA) to petrous apex lesions that are posterolateral to the paraclival segment of the internal carotid artery (ICA) requires lateralization of the paraclival segment of the ICA, carries an unignorable risk of vascular injury.
4. The contralateral transmaxillay (CTM) approach is suitable for petrous apex lesions posterolateral to the paraclival and horizontal petrous segment of the ICA, without the need to manipulate the ICA or the Eustachian tube.
5. The combined endoscopic endonasal and CTM approaches take advantage of multiport approaches with enhanced surgical freedom and provide more options in case of a vascular injury.
6. The CTM approach does not appear to add significant morbidity. The most common risks are infraorbital nerve hypesthesia and an oral-antral fistula.
7. Identification and preservation of the infraorbital nerve decrease the risk of infraorbital nerve hypesthesia.
8. A clear cut and good suture of the sublabial incision decreases the risk of oral-antral fistula.
9. The neuronavigation, mini-Doppler ultrasound, and extraocular EMG monitoring help identify critical anatomical and neurovascular structures in the petrous apex area.
10. The CTM corridor is longer than a transnasal corridor at its utmost reach. The extended drill bits or ultrasonic bone curettes should be prepared.
This article is part of the Topical Collection on Brain Tumors
Supplementary information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 241941 KB)
Rights and permissions
About this article

Cite this article
Shen, M., Shou, X., Zhao, Y. et al. How I do it? Resection of residual petrous apex chordoma with combined endoscopic endonasal and contralateral transmaxillary approaches. Acta Neurochir 164, 1967–1972 (2022). https://doi.org/10.1007/s00701-022-05243-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-022-05243-5