
Abstract
Background
The surgical resection of the tumor spreading into the cavernous sinus (CS) is complicated and challenging.
Method
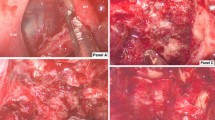
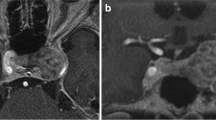
We report a left recurrent CS chondromyxoid fibroma occupying the clival-petrous apex-parasellar-suprasellar area, which was totally removed by the micro-endo combination technique via the middle cranial fossa extradural approach.
Conclusion
This case demonstrates the value of the micro-endoscopic combination technique for complicated skull base surgery.



Similar content being viewed by others

References
Chung BS, Ahn YH, Park JS (2016) Ten Triangles around Cavernous Sinus for Surgical Approach, Described by Schematic Diagram and Three Dimensional Models with the Sectioned Images. J Korean Med Sci 31:1455–1463
Dolenc VV (1985) A combined epi- and subdural direct approach to carotid-ophthalmic artery aneurysms. J Neurosurg 62:667–672
Drazin D, Wang JM, Alonso F, Patel DM, Granger A, Shoja MM, Loukas M, Oskouian RJ, Tubbs RS (2017) Intracranial Anatomical Triangles: A Comprehensive Illustrated Review. Cureus 9:e1741
Hakuba A, Liu S, Nishimura S (1986) The orbitozygomatic infratemporal approach: a new surgical technique. Surg Neurol 26:271–276
He K, Jiang S, Zhang X, Mao Y, Zhu W, Wang Y, Song J, Chen L (2018) Preliminary Exploration of the Diagnosis and Treatment of Skull-Based Chondromyxoid Fibromas. Oper Neurosurg (Hagerstown) 15:270–277
Isolan GR, Krayenbuhl N, de Oliveira E, Al-Mefty O (2007) Microsurgical Anatomy of the Cavernous Sinus: Measurements of the Triangles in and around It. Skull Base 17:357–367
Kim HS, Jee WH, Ryu KN, Cho KH, Suh JS, Cho JH, Choi YS, Lee SM, Lee JM, Sung MS, Kim JY, Jung ES, Chung YG, Ok IY (2011) MRI of chondromyxoid fibroma. Acta Radiol 52:875–880
Yasuda A, Campero A, Martins C, Rhoton AL, Jr., de Oliveira E, Ribas GC (2005) Microsurgical anatomy and approaches to the cavernous sinus. Neurosurgery 56:4–27; discussion 24–27
Zabramski JM, Kiris T, Sankhla SK, Cabiol J, Spetzler RF (1998) Orbitozygomatic craniotomy. Technical note. J Neurosurg 89:336–341
Acknowledgements
This study was sponsored Shanghai Rising-Star Program (18QA1400900) and CAMS Innovation Fund for Medical Sciences (CIFMS, 2019-I2M-5-008). The authors thank Jianbin Shi for brain imaging processing and Geng Xu for intraoperative electrophysiological monitoring support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure of potential conflicts of interest
None.
Research involving Human Participants
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by Huashan Hospital Institutional Review Board (HIRB), Fudan University, Shanghai, China.
Informed consent
It represents a video of a surgical case. The patient gave approval for this publication.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
1. The CS tumor resection is highly challenging because of the complicated neurovascular relationships.
2. The CS has four dural walls surrounding a venous plexus that receives the tributaries of multiple veins drainage.
3. Knowing the extradural and intradural triangles of the CS is essential for CS tumor operation.
4. The CMF is a rare tumor with extensive skull base involvement.
5. The orbitozygomatic extradural approach is a standard skull base technique to access the CS.
6. The Doppler ultrasound probe helps locate the ICA during CS tumor resection.
7. Care should be taken not to injure the ICA, and the direct violation of the ICA by the curettage should be avoided.
8. The wide-angle endoscope helps detect and remove the tumor around the corners covered by the eroded bony structure.
9. Since the dura is intact, gradually “pushing” the paraseller and suprasellar CMF out to the surgical cavity is useful to ease tumor removal.
10. The micro-endoscopic combination technique is helpful in selected complicated skull base surgery.
This article is part of the Topical Collection on Brain Tumors
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 105750 KB)
Rights and permissions
About this article

Cite this article
Yang, Z., Cai, J., Du, Z. et al. How I do it: Surgical Resection of a Recurrent Chondromyxoid Fibroma by Micro-Endoscopic Combination Technique. Acta Neurochir 164, 1961–1965 (2022). https://doi.org/10.1007/s00701-022-05185-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-022-05185-y