
Abstract
Background
Recognition of the right surgical cleavage plane of a vestibular schwannoma is mandatory to preserve the facial nerve function.
Method
We describe here our surgical technique that is focused on soft tissues preservation and on subperineural dissection, avoiding direct exposure of the acoustico-facial complex in order to preserve facial nerve function.
Conclusion
Soft tissue dissection helps in reducing patient’s postoperative discomfort. Meticulously keeping a subperineural plan of dissection enables to preserve facial nerve function while offering satisfying resection rates.






Similar content being viewed by others


References
Campero A, Martins C, Rhoton A, Tatagiba M (2011) Dural landmark to locate the internal auditory canal in large and giant vestibular schwannomas: the Tübingen line. Neurosurgery. https://doi.org/10.1227/NEU.0b013e31821664c6
Chibbaro S, Cebula H, Scibilia S, Spatola G, Todeschi J, Gubian A (2018) Retrosigmoid approach: investigating the role of a C-shaped skin incision and muscle flaps in improving functional outcome and reducing postoperative pain. World Neurosurg 111:e340–e347
Kohno M, Sato H, Sora S, Miwa H, Yokoyama M (2011) Is an acoustic neuroma an epiarachnoid or subarachnoid tumor? Neurosurgery 68(4):1006–1017
Lescanne E, François P, Bakhos D, Velut S, Robier A, Pollak A (2008) Vestibular schwannoma: dissection of the tumor and arachnoidal duplication. Otol Neurotol 29(7):989–994
Sasaki T, Shono T, Hashiguchi K, Yoshida F, Suzuki SO (2009) Histological considerations of the cleavage plane for preservation of facial and cochlear nerve functions in vestibular schwannoma surgery: clinical article. J Neurosurg 110(4):648–655
Starnoni D, Giammattei L, Cossu G et al (2020) Surgical management for large vestibular schwannomas: a systematic review, meta-analysis, and consensus statement on behalf of the EANS skull base section. Acta Neurochir 162(11):2595–2617
Tomio R, Yoshida K, Kohno M, Kamamoto D, Mikami S (2016) The outermost “dura-like membrane” of vestibular schwannoma. Surg Neurol Int. https://doi.org/10.4103/2152-7806.185008
Troude L, Boucekine M, Montava M, Lavieille J-P, Régis J-M, Roche P-H (2018) Adjunctive gamma knife surgery or wait and scan policy after optimal resection of large vestibular schwannomas: clinical and radiologic outcomes. World Neurosurg 118:e895–e905
Vellutini EAS, Beer-Furlan A, Brock RS, Gomes MQT, Stamm A, Cruz OLM (2014) The extracisternal approach in vestibular schwannoma surgery and facial nerve preservation. Arq Neuropsiquiatr 72(12):925–930
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Patient consent
The patient/next of kin/guardian has consented to the submission of the case report for submission to the journal.
Conflict of interest
The authors declare no competing interests.
Additional information
Key Points
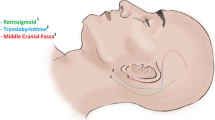
• Adequate patient’s position
• Careful soft tissues dissection to minimize patient’s postoperative discomfort
• Early cisternal opening to obtain cerebellar relaxation
• Right plane of dissection identified early at the level of the porus acusticus and kept circumferentially under continuous irrigation
• Low intensity bipolar coagulation should be used only inside the VS
• Whenever difficulties in maintaining the plane are encountered, the surgeon should change the working area
• Direct visualization of the acoustic-facial complex is avoided
• IOM is mandatory to trace the FN position and the noise of the IOM indicated maneuvers that irritate the FN
• Tumor remnants should be left onto the FN in case of tight adherences
• Adequate counselling should include patient’s expectations and possible alternative therapeutic strategies
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Tumor - Schwannoma
Supplementary information
This video represents a step by step removal of a right vestibular schwannoma. (MP4 219 mb)
Rights and permissions
About this article

Cite this article
Giammattei, L., Passeri, T., Padovan, S. et al. Vestibular schwannoma: care for soft tissues and subperineural dissection: how I do it. Acta Neurochir 163, 2247–2251 (2021). https://doi.org/10.1007/s00701-021-04801-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-021-04801-7