
Abstract
Background
If an awake surgery is somehow not available for gliomas at the language area, understanding the anatomy and well-designed surgical strategy are important.
Method
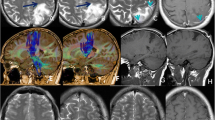
We present a case with left hemispheric multifocal high-grade gliomas located deeply at the left temporal pole, the Wernicke’s area, and mesial temporal region. Because the patient could not endure the awake surgery and obtain practicable functional magnetic resonance imaging (MRI) for eloquent cortex evaluation, we removed the lesions following the anatomical resection strategy guided by diffusion tensor imaging (DTI).
Conclusion
This case demonstrates the value of DTI and the importance of anatomical resection strategies in glioma surgeries.



Similar content being viewed by others


References
Duffau H (2007) Contribution of cortical and subcortical electrostimulation in brain glioma surgery: methodological and functional considerations. Neurophysiol Clin 37:373–382. https://doi.org/10.1016/j.neucli.2007.09.003
De Benedictis A, Sarubbo S, Duffau H (2012) Subcortical surgical anatomy of the lateral frontal region: human white matter dissection and correlations with functional insights provided by intraoperative direct brain stimulation: laboratory investigation. J Neurosurg 117:1053–1069. https://doi.org/10.3171/2012.7.JNS12628
Maldonado IL, Moritz-Gasser S, de Champfleur NM, Bertram L, Moulinie G, Duffau H (2011) Surgery for gliomas involving the left inferior parietal lobule: new insights into the functional anatomy provided by stimulation mapping in awake patients. J Neurosurg 115:770–779. https://doi.org/10.3171/2011.5.JNS112
Abdullah KG, Lubelski D, Nucifora PG, Brem S (2013) Use of diffusion tensor imaging in glioma resection. Neurosurg Focus 34:E1. https://doi.org/10.3171/2013.1.FOCUS12412
Chen F, Zhang X, Li M, Wang R, Wang HT, Zhu F, Lu DJ, Zhao H, Li JW, Xu Y, Zhu B, Zhang B (2012) Axial diffusivity and tensor shape as early markers to assess cerebral white matter damage caused by brain tumors using quantitative diffusion tensor tractography. CNS Neuroscience & Therapeutics 18:667–673. https://doi.org/10.1111/j.1755-5949.2012.00354.x
Singh G, Mehrotra A, Sardhara J, Das KK, Jamdar J, Pal L, Srivastava AK, Sahu RN, Jaiswal AK, Behari S (2015) Multiple glioblastomas: are they different from their solitary counterparts? Asian J Neurosurg 10:266–271. https://doi.org/10.4103/1793-5482.162685
Marenco-Hillembrand L, Wijesekera O, Suarez-Meade P, Mampre D, Jackson C, Peterson J, Trifiletti D, Hammack J, Ortiz K, Lesser E, Spiegel M, Prevatt C, Hawayek M, Quinones-Hinojosa A, Chaichana KL (2020) Trends in glioblastoma: outcomes over time and type of intervention: a systematic evidence based analysis. Journal of Neuro-Oncology 147:297–307. https://doi.org/10.1007/s11060-020-03451-6
Weller M, van den Bent M, Hopkins K, Tonn JC, Stupp R, Falini A, Cohen-Jonathan-Moyal E, Frappaz D, Henriksson R, Balana C, Chinot O, Ram Z, Reifenberger G, Soffietti R, Wick W (2014) EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. The Lancet Oncology 15:e395–e403. https://doi.org/10.1016/S1470-2045(14)70011-7
Lukas RV, Wainwright DA, Ladomersky E, Sachdev S, Sonabend AM, Stupp R (2019) Newly diagnosed glioblastoma: a review on clinical management. Oncology (Williston Park) 33:91–100
Acknowledgments
The DTI images in this manuscript were reconstructed using an automatic algorithm software “Diffusion Go”.
Funding
This study was supported by the Outstanding Academic Leaders Program of Shanghai Municipal Commission of Health and Family Planning (No. 2017BR006 to W.Z.), and the Shanghai Rising-Star Program (No. 18QA1400900 to J.P.S.)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Patient consent
It represents a video of a surgical case. The next of kin of the patient gave approval for this publication
Additional information
Key points
1. For high-grade gliomas, the goal of the surgery should be maximal safe resection with function preservation.
2. General anesthesia may be a rational option, if the patient cannot cooperate or tolerate the prolonged awake surgery with already-existed aphasia.
3. If an awake surgery is not available for glioma affecting language area, understanding the anatomy and well-designed surgical strategy are important.
4. A detailed preoperative neurological and neuroimaging evaluation is mandatory.
5. DTI is important to evaluate the speech-related white matter tracks and surgical approach planning.
6. The superior longitudinal fasciculus, arcuate fasciculus, and the inferior fronto-occipital fasciculus are the most important speech-related white matter tracks.
7. Anatomical resection rule is important in glioma surgeries.
8. Use transcortical approach for better deep-seated tumor exposure and subcortical neurofiber tracks preservation instead of trans-white matter methods.
9. Securing the en passage arteries before piecemeal tumor resection is the key step for tumor bleeding control.
10. Intra- and post-operative vasospasm of the en passage arteries may occur and should not be neglected.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Tumor – Glioma
Supplementary Information
701_2020_4637_MOESM1_ESM.mp4
ESM Video This video illustrates a case of multifocal high-grade glioma affecting the language area, which was successfully treated by anatomical resection in a non-awake surgery (MP4 150 mb)
Rights and permissions
About this article

Cite this article
Yang, Z., Song, J. & Zhu, W. How I do it? Anatomical multifocal high-grade glioma resection. Acta Neurochir 163, 953–957 (2021). https://doi.org/10.1007/s00701-020-04637-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-020-04637-7