
Abstract
Background
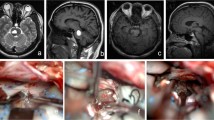
Dorsal pons cavernoma can be approached through telo-velar approach instead of transvermian approach, with lower risk of neurological deficits since it uses natural clefts to reach the floor of the fourth ventricle.
Materials and methods
We present our surgical technique for telo-velar approach to address pathologies of the dorsal pons, assisted by neuronavigation and neuromonitoring. This surgical technique is illustrated by a surgical video of a dorsal pons cavernoma.
Conclusion
Dorsal pons cavernomas can be reached through telo-velar approach after suboccipital midline craniotomy. The accurate patient positioning, cisternal dissection, and neuromonitoring use are mandatory to avoid neural injuries and identify the safe entry points into the brainstem.






Similar content being viewed by others


Abbreviations
- BAEPs:
-
Brainstem auditory evoked potentials
- mA:
-
Milliampere
- MEPs:
-
Motor evoked potentials
- MLF:
-
Median longitudinal fasciculus
- MRI:
-
Magnetic resonance imaging
- Hz:
-
Hertz
- PICA:
-
Postero-inferior-cerebellar-artery
- SSEPs:
-
Somato-sensory evoked potentials
- VA:
-
Vertebral artery
References
Garrett M, Spetzler RF (2009) Surgical treatment of brainstem cavernous malformations. Surg Neurol 72(Suppl 2):S3–S9; discussion S9-10. https://doi.org/10.1016/j.surneu.2009.05.031
Giliberto G, Lanzino DJ, Diehn FE, Factor D, Flemming KD, Lanzino G (2010) Brainstem cavernous malformations: anatomical, clinical, and surgical considerations. Neurosurg Focus 29:E9. https://doi.org/10.3171/2010.6.FOCUS10133
Mussi AC, Rhoton AL Jr (2000) Telovelar approach to the fourth ventricle: microsurgical anatomy. J Neurosurg 92:812–823. https://doi.org/10.3171/jns.2000.92.5.0812
Mussi AC, Matushita H, Andrade FG, Rhoton AL (2015) Surgical approaches to IV ventricle--anatomical study. Childs Nerv Syst 31:1807–1814. https://doi.org/10.1007/s00381-015-2809-0
Rhoton AL Jr (2000) Cerebellum and fourth ventricle. Neurosurgery 47:S7–S27. https://doi.org/10.1097/00006123-200009001-00007
Rhoton AL Jr (2000) The foramen magnum. Neurosurgery 47:S155–S193. https://doi.org/10.1097/00006123-200009001-00017
Rhoton AL Jr (2000) The posterior fossa cisterns. Neurosurgery 47:S287–S297. https://doi.org/10.1097/00006123-200009001-00029
Wang CC, Liu A, Zhang JT, Sun B, Zhao YL (2003) Surgical management of brain-stem cavernous malformations: report of 137 cases. Surg Neurol 59:444–454; discussion 454. https://doi.org/10.1016/s0090-3019(03)00187-3
Xie MG, Li D, Guo FZ, Zhang LW, Zhang JT, Wu Z, Meng GL, Xiao XR (2018) Brainstem cavernous malformations: surgical indications based on natural history and surgical outcomes. World Neurosurg 110:55–63. https://doi.org/10.1016/j.wneu.2017.10.121
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed consent
The patient gave his informed consent for the redaction and publication of the paper and the intraoperative video.
Additional information
Key points
• Dorsal pons cavernoma can be reached through telo-velar approach limiting the risk of cerebellar mutism.
• Patient positioning requires maximal neck flexion to well expose the cerebello-medullary fissure and to grant an easier way to the fourth ventricle floor.
• Colorado blade use for the skin opening reduces the surgery-related blood loss, without increasing the risk of wound complications.
• The bilateral opening of the cerebello-medullary fissures allows better exposure and mobilization of cerebellar tonsils, avoiding extreme cerebellar retraction during the approach.
• The use of cerebellar retractors should be maximally limited to avoid ischemic cerebellar lesions and venous stasis. The unilateral, gently, tonsils retraction could be used if a very lateral entry zone into the brainstem is required
• Neuromonitoring and fourth ventricle floor mapping are mandatory to choose the safe entry point into the brainstem and to avoid brainstem injuries.
• The incision on the brainstem entry point should be of maximum 2 mm. The way to the lesion can be later enlarged through a micro-dissector.
• The use of bipolar cauterization should be avoided for brainstem lesions since a minimal heat lesion can lead to severe neurological deficit. For the same reason, the surgeon should not coagulate and remove the hemosiderin around the cavernoma capsule in case of extracapsular bleeding.
• Watertight dural closure and respecting layers muscles and subcutis during the suture help to avoid posterior fossa approaches related complications like liquor leakage, infections and wound dehiscence.
• Performing an intraoperative MRI allows the identification of eventual residual lesion that can be eventually removed during the same surgery session.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Vascular Neurosurgery – Other
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Bonasia, S., De Trizio, I., Valci, L. et al. Sub-telo-velo-tonsillar approach to resect dorsal pons cavernoma through fourth ventricular floor opening: how I do it. Acta Neurochir 163, 1757–1761 (2021). https://doi.org/10.1007/s00701-020-04503-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-020-04503-6