
Abstract
Background
Complex aneurysm shape is a predominant risk factor for aneurysm rupture but its impact on clinical outcome after clipping remains unclear. The objective of the present study was to compare complications and morbidity after clipping of unruptured single-sac aneurysms (SSAs) and aneurysms with multiple sacs (MSAs).
Methods
A retrospective, single-center study was conducted for patients that were treated between 2010 and 2018. We analyzed surgical parameters, treatment-related complications, and morbidity, defined as any increase in the modified Rankin scale at 3-month follow-up.
Results
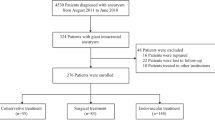
We identified 101 patients (mean age: 52.9 ± 10.5 years) that underwent clipping for 57 SSAs and 44 MSAs. The two groups were comparable regarding aneurysm size and neck width. Clipping of MSAs was associated with a longer operation time (p = 0.008) and increased use of intraoperative indocyanine green (p = 0.016) than SSAs. Complications occurred more often in the MSA group (29.5%) than in the SSA group (14.0%; p = 0.057). Morbidity was significantly higher in the MSA group (20.5%) than in the SSA group (3.5%, p = 0.009). In the univariate analysis, the odds of morbidity were 7.1 times greater for MSAs than for SSAs (95% CI 1.4–34.7).
Conclusions
Morbidity after microsurgical clipping is significantly increased in MSAs as compared to SSAs. This may be attributed to a more difficult clip placement with stronger manipulation of the aneurysm dome and the surrounding brain tissue.

Similar content being viewed by others


References
Abboud T, Rustom J, Bester M, Czorlich P, Vittorazzi E, Pinnschmidt HO, Westphal M, Regelsberger J (2017) Morphology of ruptured and unruptured intracranial aneurysms. World Neurosurg 99:610–617
André A, Boch A-L, Di Maria F, Nouet A, Sourour N, Clémenceau S, Gabrieli J, Degos V, Zeghal C, Chiras J (2018) Complication risk factors in anterior choroidal artery aneurysm treatment. Clin Neuroradiol 28:345–356
Andrews RJ, Bringas JR (1993) A review of brain retraction and recommendations for minimizing intraoperative brain injury. Neurosurgery 33:1052–1063 discussion 1063-1054
Beck J, Rohde S, El Beltagy M, Zimmermann M, Berkefeld J, Seifert V, Raabe A (2003) Difference in configuration of ruptured and unruptured intracranial aneurysms determined by biplanar digital subtraction angiography. Acta Neurochir 145:861–865
Bender MT, Wendt H, Monarch T, Lin L-M, Jiang B, Huang J, Coon AL, Tamargo RJ, Colby GP (2017) Shifting treatment paradigms for ruptured aneurysms from open surgery to endovascular therapy over 25 years. World Neurosurg 106:919–924
Borggrefe J, Behme D, Mpotsaris A, Weber W (2016) Complications associated with cerebral aneurysm morphology in balloon-assisted coil embolization of ruptured and Unruptured aneurysms—a single-center analysis of 116 consecutive cases. World Neurosurg 91:483–489
Byoun HS, Bang JS, Oh CW, Kwon OK, Hwang G, Han JH, Kim T, Lee SU, Jo SR, Kim DG, Park KS (2016) The incidence of and risk factors for ischemic complications after microsurgical clipping of unruptured middle cerebral artery aneurysms and the efficacy of intraoperative monitoring of somatosensory evoked potentials: a retrospective study. Clin Neurol Neurosurg 151:128–135
Chyatte D, Porterfield R (2001) Functional outcome after repair of unruptured intracranial aneurysms. J Neurosurg 94:417–421
Delgado AF, Andersson T, Delgado AF (2017) Clinical outcome after surgical clipping or endovascular coiling for cerebral aneurysms: a pragmatic meta-analysis of randomized and non-randomized trials with short-and long-term follow-up. J Neurointerv Surg 9:264–277
Dhar S, Tremmel M, Mocco J, Kim M, Yamamoto J, Siddiqui AH, Hopkins LN, Meng H (2008) Morphology parameters for intracranial aneurysm rupture risk assessment. Neurosurgery 63:185–197
Etminan N, Beseoglu K, Barrow DL, Bederson J, Brown RD, Connolly ES, Derdeyn CP, Hänggi D, Hasan D, Juvela S (2014) Multidisciplinary consensus on assessment of unruptured intracranial aneurysms. Stroke 45:1523–1530
Forbes G, Fox AJ, Huston J, Wiebers DO, Torner J (1996) Interobserver variability in angiographic measurement and morphologic characterization of intracranial aneurysms: a report from the international study of unruptured intracranial aneurysms. Am J Neuroradiol 17:1407–1415
Gerlach R, Beck J, Setzer M, Vatter H, Berkefeld J, de Rochemont RDM, Raabe A, Seifert V (2007) Treatment related morbidity of unruptured intracranial aneurysms: results of a prospective single centre series with an interdisciplinary approach over a 6 year period (1999–2005). J Neurol Neurosurg Psychiatry 78:864–871
Goertz L, Hamisch C, Telentschak S, Kabbasch C, von Spreckelsen N, Stavrinou P, Timmer M, Goldbrunner R, Brinker G, Krischek B (2018) Impact of aneurysm shape on intraoperative rupture during clipping of ruptured intracranial aneurysms. World Neurosurg. https://doi.org/10.1016/j.wneu.2018.07.058
Hademenos G, Massoud T, Turjman F, Sayre J (1998) Anatomical and morphological factors correlating with rupture of intracranial aneurysms in patients referred for endovascular treatment. Neuroradiology 40:755–760
Hammer A, Steiner A, Kerry G, Ranaie G, Baer I, Hammer CM, Kunze S, Steiner HH (2017) Treatment of ruptured intracranial aneurysms yesterday and now. PLoS One 12:e0172837
Hwang JS, Hyun MK, Lee HJ, Choi JE, Kim JH, Lee NR, Kwon J-W, Lee E (2012) Endovascular coiling versus neurosurgical clipping in patients with unruptured intracranial aneurysm: a systematic review. BMC Neurol 12:99
Investigators UJ (2012) The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med 2012:2474–2482
Kotowski M, Naggara O, Darsaut TE, Nolet S, Gevry G, Kouznetsov E, Raymond J (2012) Safety and occlusion rates of surgical treatment of unruptured intracranial aneurysms: a systematic review and meta-analysis of the literature from 1990 to 2011. J Neurol Neurosurg Psychiatry 84:42–48
Lall RR, Eddleman CS, Bendok BR, Batjer HH (2009) Unruptured intracranial aneurysms and the assessment of rupture risk based on anatomical and morphological factors: sifting through the sands of data. Neurosurg Focus 26:E2
Molyneux A, Group ISATC (2002) International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 360:1267–1274
Ogilvy CS, Carter BS, Kaplan S, Rich C, Crowell RM (1996) Temporary vessel occlusion for aneurysm surgery: risk factors for stroke in patients protected by induced hypothermia and hypertension and intravenous mannitol administration. J Neurosurg 84:785–791
Oh SY, Kim MJ, Kim BM, Lee KS, Kim BS, Shin YS (2013) Angiographic characteristics of ruptured paraclinoid aneurysms: risk factors for rupture. Acta Neurochir 155:1493–1499
Park JS, Kim H, Baik MW, Park IS (2017) Risk factor analysis for poor outcomes in supraorbital keyhole aneurysm clipping for ruptured anterior circulation aneurysm. World Neurosurg 111:e386–e394. https://doi.org/10.1016/j.wneu.2017.12.071
Teo M, Martin S, Ponweera A, Macey A, Suttner N, Brown J, St George J (2015) Results of surgical clipping in a neurointerventional dominant department. Br J Neurosurg 29:792–798
Wang JT, Yang HC, Lin CF, Guo WY, Luo CB, Chen MH, Hsu SP (2014) Bilobulated paraclinoid aneurysm mimics double aneurysms: a comparison of endovascular coiling and surgical clipping treatments. J Chin Med Assoc 77:544–547
Wiebers DO, Investigators ISUIA (2003) Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 362:103–110
Zhao J, Lin H, Summers R, Yang M, Cousins BG, Tsui J (2018) Current treatment strategies for intracranial aneurysms: an overview. Angiology 69:17–30
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
For this type of study, formal consent is not required.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
This article is part of the Topical Collection on Vascular Neurosurgery - Aneurysm
Rights and permissions
About this article

Cite this article
Goertz, L., Kasuya, H., Hamisch, C. et al. Impact of aneurysm shape on morbidity after clipping of unruptured intracranial aneurysms. Acta Neurochir 160, 2169–2176 (2018). https://doi.org/10.1007/s00701-018-3675-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-018-3675-9