
Abstract
Background
Pituitary adenomas are usually considered benign tumours, although some of them can exhibit an aggressive behaviour. Patients with clinically aggressive pituitary adenomas are frequently diagnosed with larger masses, and may present an earlier recurrence (or persistence) after surgery. Our aim was to characterise the clinical, histopathological and radiological features of patients with aggressive pituitary adenoma, in order to correlate their clinical behaviour with the response to treatment plan.
Method
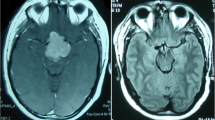
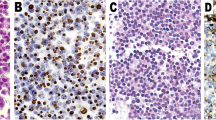
We considered an aggressive pituitary adenoma on the basis of radiological features (size, local invasion), pathological reports (atypical adenoma: MIB-1 >3%, p53 immunoreactivity, increased mitotic activity) and clinical aspects (response to surgery, radiotherapy and medical treatment).
Results
Among our cohort of 582 patients, we considered 102 subjects with aggressive pituitary adenomas (18%, 56 male and 46 female): 14 adrenocorticotrophic hormone (ACTH)-secreting, 18 growth hormone (GH)-secreting, 23 prolactin (PRL)-secreting and 47 non-secreting, with a median follow-up of 5 years. In the whole cohort, 75% of patients with aggressive pituitary adenomas presented invasion of surrounding structure, especially GH-secreting, PRL-secreting and non-secreting. Besides invasion, their remission rate after surgery, radiotherapy or medical treatment was similar, irrespective of hormonal secretion. Surgery was the most performed treatment (overall remission rate of 24%), especially in those patients with ACTH- or GH-secreting adenoma, and 22% of patients were submitted to radiotherapy, with a remission rate of 45% after a median of 3 years. Two consecutive years of medical treatment, in patients with secreting pituitary adenoma, achieved disease control in 41% of them. Considering pathological reports, 24% of cases were defined as atypical adenomas; radiological characteristics, responses to medical treatment and remission rates were similar among patients with typical and atypical adenoma.
Conclusions
We proposed a new and comprehensive definition of aggressive pituitary adenoma, based upon radiological, clinical and pathological features. In a selected cohort of patients, radiological invasion resulted in the most common marker to describe the aggressive behaviour of pituitary adenoma. Surgery, radiotherapy and medical treatment (the latter only in secreting adenoma) achieved disease control in half of the patients with aggressive adenoma, especially surgery in those with ACTH-oma and medical treatment in those with GH- and PRL-secreting adenoma. Nevertheless, radiological, clinical or atypical features did not affect the outcome.
Similar content being viewed by others

References
Ceccato F, Occhi G, Regazzo D, Randi ML, Cecchin D, Gardiman MP, Manara R, Lombardi G, Denaro L, Mantero F, Scaroni C (2014) Gonadotropin secreting pituitary adenoma associated with erythrocytosis: case report and literature review. Hormones 13(1):131
Ceccato F, Lombardi G, Manara R, Emanuelli E, Denaro L, Milanese L, Gardiman MP, Bertorelle R, Scanarini M, D’Avella D, Occhi G, Boscaro M, Zagonel V, Scaroni C (2015) Temozolomide and pasireotide treatment for aggressive pituitary adenoma: expertise at a tertiary care center. J Neuro-Oncol 122(1):189–196
Chatzellis E, Alexandraki KI, Androulakis II, Kaltsas G (2015) Aggressive pituitary tumors. Neuroendocrinology 101(2):87–104
Daly AF, Rixhon M, Adam C, Dempegioti A, Tichomirowa MA, Beckers A (2006) High prevalence of pituitary adenomas: a cross-sectional study in the province of Liege, Belgium. J Clin Endocrinol Metab 91(12):4769–4775
De Lellis RA, Lloyd RV, Heitz PU, Eng C (2004) World Health Organization classification of tumours: tumours of endocrine organs. IARC, Lyon
Di Ieva A, Rotondo F, Syro LV, Cusimano MD, Kovacs K (2014) Aggressive pituitary adenomas-diagnosis and emerging treatments. Nat Rev Endocrinol 10(7):423–435
Han S, Gao W, Jing Z, Wang Y, Wu A (2017) How to deal with giant pituitary adenomas: transsphenoidal or transcranial, simultaneous or two-staged? J Neuro-Oncol 132:313–321
Katznelson L, Laws ER Jr, Melmed S, Molitch ME, Murad MH, Utz A, Wass JA (2014) Acromegaly: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 99(11):3933–3951
Losa M, Picozzi P, Motta M, Valle M, Franzin A, Mortini P (2011) The role of radiation therapy in the management of non-functioning pituitary adenomas. J Endocrinol Investig 34(8):623–629
Losa M, Bogazzi F, Cannavo S, Ceccato F, Curtò L, De Marinis L, Iacovazzo D, Lombardi G, Mantovani G, Mazza E, Minniti G, Nizzoli M, Reni M, Scaroni C (2016) Temozolomide therapy in patients with aggressive pituitary adenomas or carcinomas. J Neuro-Oncol 126(3):519–525
Manara R, Maffei P, Citton V, Rizzati S, Bommarito G, Ermani M, Albano I, Della Puppa A, Carollo C, Pavesi G, Scanarini M, Ceccato F, Sicolo N, Mantero F, Scaroni C, Martini C (2011) Increased rate of intracranial saccular aneurysms in acromegaly: an MR angiography study and review of the literature. J Clin Endocrinol Metab 96(5):1292–1300
Melmed S, Casanueva FF, Hoffman AR, Kleinberg DL, Montori VM, Schlechte JA, Wass JA (2011) Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 96(2):273–288
Mindermann T, Wilson CB (1994) Age-related and gender-related occurrence of pituitary adenomas. Clin Endocrinol 41:359–364
Nieman LK, Biller BM, Findling JW, Murad MH, Newell-Price J, Savage MO, Tabarin A (2015) Treatment of Cushing’s Syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 100(8):2807–2831
Nomikos P, Buchfelder M, Fahlbusch R (2005) The outcome of surgery in 668 patients with acromegaly using current criteria of biochemical ‘cure’. Eur J Endocrinol 152:379–387
Pawlikowski M, Radek M, Kunert-Radek J, Jaranowska M, Świętosławski J, Winczyk K (2014) Overexpression of prothymosin alpha is related to pituitary adenoma recurrence but not to adenoma invasiveness and proliferation. Endokrynol Pol 65(5):382–386
Saeger W, Lüdecke DK, Buchfelder M, Fahlbusch R, Quabbe HJ, Petersenn S (2007) Pathohistological classification of pituitary tumors: 10 years of experience with the German pituitary tumor registry. Eur J Endocrinol 156(2):203–216
Saeger W, Petersenn S, Schöfl C, Knappe UJ, Theodoropoulou M, Buslei R, Honegger J (2016) Emerging histopathological and genetic parameters of pituitary adenomas: clinical impact and recommendation for future WHO classification. Endocr Pathol 27:115–122
Saeki N, Yamaura A, Numata T (1999) Transsphenoidal reoperations for removal of pituitary adenomas: rhinological management and timing of reoperation. J Clin Neurosci 6:385–388
Sav A, Rotondo F, Syro LV, Di Ieva A, Cusimano MD, Kovacs K (2015) Invasive, atypical and aggressive pituitary adenomas and carcinomas. Endocrinol Metab Clin N Am 44:99–104
Salenave S, Boyce AM, Collins MT, Chanson P (2014) Acromegaly and McCune-Albright syndrome. J Clin Endocrinol Metab 99:1955–1969
Shimon I, Jallad RS, Fleseriu M, Yedinak CG, Greenman Y, Bronstein MD (2015) Giant GH-secreting pituitary adenomas: management of rare and aggressive pituitary tumors. Eur J Endocrinol 172:707–713
Vieira JO Jr, Cukiert A, Liberman B (2006) Evaluation of magnetic resonance imaging criteria for cavernous sinus invasion in patients with pituitary adenomas: logistic regression analysis and correlation with surgical findings. Surg Neurol 65:130–135
Wang J, Voellger B, Benzel J, Schlomann U, Nimsky C, Bartsch JW, Carl B (2016) Metalloproteinases ADAM12 and MMP-14 are associated with cavernous sinus invasion in pituitary adenomas. Int J Cancer 139:1327–1339
Zada G, Woodmansee WW, Ramkissoon S, Amadio J, Nose V, Laws ER (2011) A typical pituitary adenomas: incidence, clinical characteristics, and implications. J Neurosurg 114:336–344
Zilio M, Barbot M, Ceccato F, Camozzi V, Bilora F, Casonato A, Frigo AC, Albiger N, Daidone V, Mazzai L, Mantero F, Scaroni C (2014) Diagnosis and complications of Cushing's disease: gender-related differences. Clin Endocrinol 80:403–410
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Ceccato, F., Regazzo, D., Barbot, M. et al. Early recognition of aggressive pituitary adenomas: a single-centre experience. Acta Neurochir 160, 49–55 (2018). https://doi.org/10.1007/s00701-017-3396-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-017-3396-5