
Abstract
Background
Tumors of the middle fossa or cavernous sinus (CS), or intraorbital tumors, can penetrate each other through the superior orbital fissure (SOF) or neighboring tissue. These complicated pathologies are often treated with highly invasive surgical procedures. In this article, we demonstrate surgical anatomic dissections of the CS, SOF, orbital apex (OA), and dura mater extending to the periorbita from the middle fossa, by performing an epidural dissection via a lateral orbitotomy approach, and discuss findings that may provide guidance during surgery in these regions.
Methods
Lateral orbitotomy was performed on latex-injected cadaver heads by making a 2-cm skin incision lateral to the lateral canthus, drilling the lesser and greater sphenoid wings that form the SOF borders, and removing the bone section between the middle fossa and orbit. Dura mater from the middle fossa to the periorbita was exposed to perform anterior clinoidectomy. Meningeal dura was dissected from the endosteal dura, which forms the lateral wall of the CS, to expose the CS, SOF, and OA for dissections.
Results
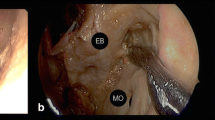
Changing the orientation of the microscope from posterior to anterior enabled regional control for dissection from the Gasserian ganglion to the OA. Cranial nerves that pass through the CS, SOF, and OA were dissected and exposed. The annular tendon was opened, revealing the oculomotor nerves and its branches, as well as the abducens and nasociliary nerves, which pass through the oculomotor foramen and course within the OA and orbit.
Conclusions
This approach causes less tissue damage; provides control of the surgical area in spheno-orbital tumors invading the fissure and foramen by changing the orientation of the microscope toward the orbit, OA, SOF, CS, and middle fossa; and expands the indication criteria for lateral orbitotomy surgery. This approach, therefore, represents an alternative surgical method for excising complicated tumors in these regions.













Similar content being viewed by others


References
Abdel Aziz KM, Bhatia S, Tantawy MH, Sekula R, Keller JT, Froelich S, Happ E (2011) Minimally invasive transpalpebral “eyelid” approach to the anterior cranial base. Neurosurgery 69:ons195–206; discussion 206-197
Altay T, Patel BC, Couldwell WT (2012) Lateral orbital wall approach to the cavernous sinus. J Neurosurg 116:755–763
Arai H, Sato K, Katsuta T, Rhoton AL Jr (1996) Lateral approach to intraorbital lesions: anatomic and surgical considerations. Neurosurgery 39:1157–1162, discussion 1162-1153
Dolenc V (1999) Extradural approach to intracavernous ICA aneurysms. In: Reulen H-J (ed) Neurosurgical management of aneurysmal subarachnoid haemorrhage. Acta neurochirgica supplements, vol 72. Springer, Verlag Wien, Vienna, pp 99–106
Dolenc VV (1989) Anatomy and surgery of the cavernous sinus. Springer-Verlag Wien, New York
Dolenc VV (1997) Transcranial epidural approach to pituitary tumors extending beyond the sella. Neurosurgery 41:542–552
Dolenc VV (1999) A combined transorbital-transclinoid and transsylvian approach to carotid-ophthalmic aneurysms without retraction of the brain. In: Reulen H-J (ed) Neurosurgical management of aneurysmal subarachnoid haemorrhage. Acta neurochirurgica supplement, vol 72. Springer, Verlag Wien, Vienna, pp 89–97
Dolenc VV (2003) Microsurgical anatomy and surgery of the central skull base. Springer-Verlag Wien, New York
Fries G, Perneczky A (1998) Endoscope-assisted brain surgery: part 2–analysis of 380 procedures. Neurosurgery 42:226–231, discussion 231-222
Hakuba A, Matsuoka Y, Suzuki T, Komiyama M, Jin T, Inoue Y (1987) Direct approaches to vascular lesions in the cavernous sinus via the medial triangle. In: Dolenc VV (ed) The cavernous sinus. Springer, Verlag Wien, Vienna, pp 272–284
Jho HD (1997) Orbital roof craniotomy via an eyebrow incision: a simplified anterior skull base approach. Minim Invasive Neurosurg 40:91–97
Lesoin F, Pellerin P, Autrique A, Clarisse J, Jomin M (1987) The direct microsurgical approach to intracavernous tumors. In: Dolenc VV (ed) The cavernous sinus. Springer, Verlag Wien, Vienna, pp 323–331
Mariniello G, Maiuri F, de Divitiis E, Bonavolonta G, Tranfa F, Iuliano A, Strianese D (2010) Lateral orbitotomy for removal of sphenoid wing meningiomas invading the orbit. Neurosurgery 66:287–292, discussion 292
Maroon JC, Kennerdell JS (1976) Lateral microsurgical approach to intraorbital tumors. J Neurosurg 44:556–561
Maroon JC, Kennerdell JS (1984) Surgical approaches to the orbit. Indications and techniques. J Neurosurg 60:1226–1235
Natori Y, Rhoton AL Jr (1994) Transcranial approach to the orbit: microsurgical anatomy. J Neurosurg 81:78–86
Natori Y, Rhoton AL Jr (1995) Microsurgical anatomy of the superior orbital fissure. Neurosurgery 36:762–775
Ouyang T, Zhang N, Wang L, Li Z, Chen J (2015) Sphenoid wing meningiomas: surgical strategies and evaluation of prognostic factors influencing clinical outcomes. Clin Neurol Neurosurg 134:85–90
Perneczky A, Fries G (1998) Endoscope-assisted brain surgery: part 1–evolution, basic concept, and current technique. Neurosurgery 42:219–224, discussion 224-215
Pieper DR, A-MO (1999) Cranio-orbito-zygomatic approach. Operat Tech Neurosurg 2:2–9
Reisch R, Marcus HJ, Hugelshofer M, Koechlin NO, Stadie A, Kockro RA (2014) Patients’ cosmetic satisfaction, pain, and functional outcomes after supraorbital craniotomy through an eyebrow incision. J Neurosurg 121:730–734
Rhoton AL Jr (2002) The cavernous sinus, the cavernous venous plexus, and the carotid collar. Neurosurgery 51:S375–S410
Rhoton AL Jr (2002) The orbit. Neurosurgery 51:S303–S334
Ringel F, Cedzich C, Schramm J (2007) Microsurgical technique and results of a series of 63 spheno-orbital meningiomas. Neurosurgery 60:214–221, discussion 221-212
Roth J, Fraser JF, Singh A, Bernardo A, Anand VK, Schwartz TH (2011) Surgical approaches to the orbital apex: comparison of endoscopic endonasal and transcranial approaches using a novel 3D endoscope. Orbit 30:43–48
Steiger HJ, Schmid-Elsaesser R, Stummer W, Uhl E (2001) Transorbital keyhole approach to anterior communicating artery aneurysms. Neurosurgery 48:347–351, discussion 351-342
van Lindert E, Perneczky A, Fries G, Pierangeli E (1998) The supraorbital keyhole approach to supratentorial aneurysms: concept and technique. Surg Neurol 49:481–489, discussion 489–490
Yasuda A, Campero A, Martins C, Rhoton AL Jr, de Oliveira E, Ribas GC (2008) Microsurgical anatomy and approaches to the cavernous sinus. Neurosurgery 62:1240–1263
Acknowledgments
Thanks to Nurdan Ulutas for drawings.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for this research.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
Ethical approval was not required for this type of study at our institute.
Additional information
Comments
This article applies in full extent to the principles of pterional epidural approach to cavernous sinus and orbital apex pioneered by Vinko Dolenc 25 years ago (1). These principles are applied here in cadaver study by minimally invasive route using lateral orbitotomy approach and by turning microscope from anterior (toward orbital apex) to posterior directions (toward CS and middle fossa). As surgery in this complex anatomical part of the central skull base is extremely demanding and includes serious morbidities (2), mostly not accepted anymore nowadays and thus treated in a different way, such cadaver study is not only an excellent repetition of parasellar microanatomy but also stresses out the key questions on very narrow indications and very serious limitations of some minimally invasive approaches versus more traditional ones.
Roman Bosnjak
Ljubljana, Slovenia
1. Dolenc VV. Anatomy and surgery of the cavernous sinus New York, Dordrecht, Heidelberg, London: Springer-Verlag; 1989
2. Dolenc V V. Microsurgical Anatomy and Surgery of the Central Skull Base. Wien, Austria: Springer-Verlag; 2003.
The authors present a nice anatomical description of the lateral orbitotomy with extended variations exposing the clinoidal region, cavernous sinus, SOF, and the Gasserian ganglion. There is a natural access to the sphenoid bone and fronto-temporal region when the lateral orbital wall is removed between frontozygomatic process and orbitozygomatic junction, and as it is shown, a relative wide exposure can be achieved. The lack of clinical experience makes this paper less attractive, however this is a nice anatomical effort to expose this region in a rather minimally access way. Yet, although the proximal control of carotid can be achieved in the clinoidal segment, this approach is not optimal for tackling ophthalmic artery aneurysms while having a temporary clip positioned in the clinoid segment. The visualization might be limited. For other lesions, and specifically if the goal is a biopsy or subtotal resection, the approach could be very appropriate. Skull base surgeons should get familiar with this minimally access exposure, and get appropriate exposure and knowledge about this alternative with cadaveric dissection.
Amir Dehdashti
NY, USA
Rights and permissions
About this article

Cite this article
Ulutas, M., Boyacı, S., Akakın, A. et al. Surgical anatomy of the cavernous sinus, superior orbital fissure, and orbital apex via a lateral orbitotomy approach: a cadaveric anatomical study. Acta Neurochir 158, 2135–2148 (2016). https://doi.org/10.1007/s00701-016-2940-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-016-2940-z