
Abstract
Background
Intraoperative MRI (iMRI) increases gross total resection (GTR) rates in transsphenoidal surgery; however, long-term follow-up data is lacking. The objective is to assess the outcome of patients with nonfunctioning pituitary adenomas (NFA) at a mean follow-up of > 5 years.
Methods
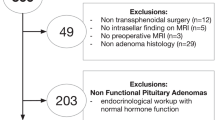
Patients with NFA operated in a single institution with resection control by a 1.5 T intraoperative magnetic resonance imaging (iMRI) scanner and no previous pituitary surgery were included. Microscopical transsphenoidal approaches with optional endoscopy were used. The iMRI was chosen for spacious suprasellar or retrosellar and/or invasive tumours. IMRI-scans were made if GTR or if nonresectable remnants were presumed. The patients had a full neuroradiological, endocrinological and ophthalmological follow-up at the institution.
Results
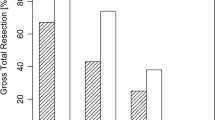
Eighty-five patients (67 % male;55 ± 14 years) with a follow-up of 5.6 ± 1.9 years were included. The initial GTR rate on iMRI was 44 %. In 83 %, further resections were possible, resulting in a final GTR rate of 66 %. In invasive tumours, the GTR rate was increased by 29 %. The detection of remnants by iMRI had high sensitivity and specificity (100 %), as opposed to endoscopy (21 %;78 %). During follow-up, four (7 %) tumours recurred and 14 (64 %) remnants grew. The recurrence and regrowth rate were 0.013 and 0.114 patients/years, respectively. Seventy-nine percent of the growing remnants were seen < 5 years postoperatively.
Conclusions
The use of iMRI for transsphenoidal resection leads to low recurrence rates. Even in case of invasive tumours, distinctly more patients show long tumour-free follow-ups. Tumour remnants detected by iMRI are at high risk to grow within 5 years after surgery.

Similar content being viewed by others

References
Abosch A, Tyrrell JB, Lamborn KR, Hannegan LT, Applebury CB, Wilson CB (1998) Transsphenoidal microsurgery for growth hormone-secreting pituitary adenomas: initial outcome and long-term results. J Clin Endocrinol Metab 83:3411–3418
Ahn JY, Jung JY, Kim J, Lee KS, Kim SH (2008) How to overcome the limitations to determine the resection margin of pituitary tumours with low-field intra-operative MRI during trans-sphenoidal surgery: usefulness of Gadolinium-soaked cotton pledgets. Acta Neurochir (Wien) 150:763–771, discussion 771
Albayrak B, Samdani AF, Black PM (2004) Intra-operative magnetic resonance imaging in neurosurgery. Acta Neurochir (Wien) 146:543–556, discussion 557
Arafah BM (1986) Reversible hypopituitarism in patients with large nonfunctioning pituitary adenomas. J Clin Endocrinol Metab 62:1173–1179
Barker FG 2nd, Klibanski A, Swearingen B (2003) Transsphenoidal surgery for pituitary tumors in the United States, 1996–2000: mortality, morbidity, and the effects of hospital and surgeon volume. J Clin Endocrinol Metab 88:4709–4719
Baskin DS, Boggan JE, Wilson CB (1982) Transsphenoidal microsurgical removal of growth hormone-secreting pituitary adenomas. A review of 137 cases. J Neurosurg 56:634–641
Baumann F, Schmid C, Bernays RL (2010) Intraoperative magnetic resonance imaging-guided transsphenoidal surgery for giant pituitary adenomas. Neurosurg Rev 33:83–90
Bellut D, Hlavica M, Muroi C, Woernle CM, Schmid C, Bernays RL (2012) Impact of intraoperative MRI-guided transsphenoidal surgery on endocrine function and hormone substitution therapy in patients with pituitary adenoma. Swiss Med Wkly 142:w13699
Bellut D, Hlavica M, Schmid C, Bernays RL (2010) Intraoperative magnetic resonance imaging-assisted transsphenoidal pituitary surgery in patients with acromegaly. Neurosurg Focus 29:E9
Berg C, Meinel T, Lahner H, Mann K, Petersenn S (2010) Recovery of pituitary function in the late-postoperative phase after pituitary surgery: results of dynamic testing in patients with pituitary disease by insulin tolerance test 3 and 12 months after surgery. Eur J Endocrinol 162:853–859
Berkmann S, Fandino J, Muller B, Kothbauer K, Henzen C, Landolt H (2012) Pituitary surgery: experience from a large network in Central Switzerland. Swiss medical weekly 142:0
Berkmann S, Fandino J, Muller B, Remonda L, Landolt H (2012) Intraoperative MRI and endocrinological outcome of transsphenoidal surgery for non-functioning pituitary adenoma. Acta Neurochir (Wien) 154:639–647
Berkmann S, Fandino J, Zosso S, Killer HE, Remonda L, Landolt H (2011) Intraoperative magnetic resonance imaging and early prognosis for vision after transsphenoidal surgery for sellar lesions. J Neurosurg 115:518–527
Berkmann S, Schlaffer S, Buchfelder M (2013) Tumor shrinkage after transsphenoidal surgery for nonfunctioning pituitary adenoma. J Neurosurg 119(6):1447–1452
Black PM, Moriarty T, Alexander E 3rd, Stieg P, Woodard EJ, Gleason PL, Martin CH, Kikinis R, Schwartz RB, Jolesz FA (1997) Development and implementation of intraoperative magnetic resonance imaging and its neurosurgical applications. Neurosurgery 41:831–842, discussion 842–835
Bohinski RJ, Warnick RE, Gaskill-Shipley MF, Zuccarello M, van Loveren HR, Kormos DW, Tew JM Jr (2001) Intraoperative magnetic resonance imaging to determine the extent of resection of pituitary macroadenomas during transsphenoidal microsurgery. Neurosurgery 49:1133–1143, discussion 1143–1134
Bradley KJ, Wass JA, Turner HE (2003) Non-functioning pituitary adenomas with positive immunoreactivity for ACTH behave more aggressively than ACTH immunonegative tumours but do not recur more frequently. Clin Endocrinol (Oxf) 58:59–64
Brochier S, Galland F, Kujas M, Parker F, Gaillard S, Raftopoulos C, Young J, Alexopoulou O, Maiter D, Chanson P (2010) Factors predicting relapse of nonfunctioning pituitary macroadenomas after neurosurgery: a study of 142 patients. Eur J Endocrinol 163:193–200
Buchfelder M, Schlaffer S-M (2012) Intraoperative magnetic resonance imaging during surgery for pituitary adenomas: pros and cons. Endocrine 42:483–495
Bulters DO, Shenouda E, Evans BT, Mathad N, Lang DA (2009) Visual recovery following optic nerve decompression for chronic compressive neuropathy. Acta Neurochir (Wien) 151:325–334
Cappabianca P, Cavallo LM, Colao A, de Divitiis E (2002) Surgical complications associated with the endoscopic endonasal transsphenoidal approach for pituitary adenomas. J Neurosurg 97:293–298
Cho HY, Cho SW, Kim SW, Shin CS, Park KS, Kim SY (2010) Silent corticotroph adenomas have unique recurrence characteristics compared with other nonfunctioning pituitary adenomas. Clin Endocrinol (Oxf) 72:648–653
Ciric I, Ragin A, Baumgartner C, Pierce D (1997) Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience. Neurosurgery 40:225–236, discussion 236–227
Coburger J, Konig R, Seitz K, Bazner U, Wirtz CR, Hlavac M (2013) Determining the utility of intraoperative magnetic resonance imaging for transsphenoidal surgery: a retrospective study. J Neurosurg 120(2):346–356
Cohen AR, Cooper PR, Kupersmith MJ, Flamm ES, Ransohoff J (1985) Visual recovery after transsphenoidal removal of pituitary adenomas. Neurosurgery 17:446–452
Colao A, Cerbone G, Cappabianca P, Ferone D, Alfieri A, Di Salle F, Faggiano A, Merola B, de Divitiis E, Lombardi G (1998) Effect of surgery and radiotherapy on visual and endocrine function in nonfunctioning pituitary adenomas. J Endocrinol Invest 21:284–290
Comtois R, Beauregard H, Somma M, Serri O, Aris-Jilwan N, Hardy J (1991) The clinical and endocrine outcome to trans-sphenoidal microsurgery of nonsecreting pituitary adenomas. Cancer 68:860–866
Darakchiev BJ, Tew JM Jr, Bohinski RJ, Warnick RE (2005) Adaptation of a standard low-field (0.3-T) system to the operating room: focus on pituitary adenomas. Neurosurg Clin N Am 16:155–164
De Witte O, Makiese O, Wikler D, Levivier M, Vandensteene A, Pandin P, Baleriaux D, Brotchi J (2005) Transsphenoidal approach with low field MRI for pituitary adenoma. Neurochirurgie 51:577–583
Dekkers OM, Pereira AM, Romijn JA (2008) Treatment and follow-up of clinically nonfunctioning pituitary macroadenomas. J Clin Endocrinol Metab 93:3717–3726
Dort JC, Sutherland GR (2001) Intraoperative magnetic resonance imaging for skull base surgery. Laryngoscope 111:1570–1575
Ebersold MJ, Quast LM, Laws ER Jr, Scheithauer B, Randall RV (1986) Long-term results in transsphenoidal removal of nonfunctioning pituitary adenomas. J Neurosurg 64:713–719
Fahlbusch R, Ganslandt O, Buchfelder M, Schott W, Nimsky C (2001) Intraoperative magnetic resonance imaging during transsphenoidal surgery. J Neurosurg 95:381–390
Fahlbusch R, Keller B, Ganslandt O, Kreutzer J, Nimsky C (2005) Transsphenoidal surgery in acromegaly investigated by intraoperative high-field magnetic resonance imaging. Eur J Endocrinol 153:239–248
Faria MA Jr, Tindall GT (1982) Transsphenoidal microsurgery for prolactin-secreting pituitary adenomas. J Neurosurg 56:33–43
Fatemi N, Dusick JR, Mattozo C, McArthur DL, Cohan P, Boscardin J, Wang C, Swerdloff RS, Kelly DF (2008) Pituitary hormonal loss and recovery after transsphenoidal adenoma removal. Neurosurgery 63:709–718, discussion 718–709
Findlay G, McFadzean RM, Teasdale G (1983) Recovery of vision following treatment of pituitary tumours; application of a new system of assessment to patients treated by transsphenoidal operation. Acta Neurochir (Wien) 68:175–186
Freda PU, Beckers AM, Katznelson L, Molitch ME, Montori VM, Post KD, Vance ML, Endocrine S (2011) Pituitary incidentaloma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 96:894–904
Gerlach R, du Mesnil de Rochemont R, Gasser T, Marquardt G, Reusch J, Imoehl L, Seifert V (2008) Feasibility of Polestar N20, an ultra-low-field intraoperative magnetic resonance imaging system in resection control of pituitary macroadenomas: lessons learned from the first 40 cases. Neurosurgery 63:272–284, discussion 284–275
Greenman Y, Stern N (2009) How should a nonfunctioning pituitary macroadenoma be monitored after debulking surgery? Clin Endocrinol (Oxf) 70:829–832
Hardy J, Wigser SM (1965) Transsphenoidal surgery of pituitary fossa tumors with televised radiofluoroscopic control. J Neurosurg 23:612–619
Harris PE, Afshar F, Coates P, Doniach I, Wass JA, Besser GM, Grossman A (1989) The effects of transsphenoidal surgery on endocrine function and visual fields in patients with functionless pituitary tumours. Q J Med 71:417–427
Hlavica M, Bellut D, Lemm D, Schmid C, Bernays RL (2013) Impact of ultra-low-field intraoperative magnetic resonance imaging on extent of resection and frequency of tumor recurrence in 104 surgically treated nonfunctioning pituitary adenomas. World Neurosurg 79:99–109
Jane JA Jr, Laws ER Jr (2010) Endoscopy versus MR imaging. J Neurosurg 112:734, discussion 735
Jones J, Ruge J (2007) Intraoperative magnetic resonance imaging in pituitary macroadenoma surgery: an assessment of visual outcome. Neurosurg Focus 23:E12
Karavitaki N (2012) Prevalence and incidence of pituitary adenomas. Ann Endocrinol (Paris) 73:79–80
Knosp E, Steiner E, Kitz K, Matula C (1993) Pituitary adenomas with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with surgical findings. Neurosurgery 33:610–617, discussion 617–618
Lang MJ, Kelly JJ, Sutherland GR (2011) A moveable 3-Tesla intraoperative magnetic resonance imaging system. Neurosurgery 68:168–179
Laws ER Jr, Ebersold MJ, Piegras DG (1982) The results of transsphenoidal surgery in specific clinical entities. In: Laws ER, Randall RV, Kern EB et al (eds) Management of Pituitary Adenomas and Related Lesions with Emphasis on Transsphenoidal Microsurgery. Appleton-Century-Crofts, New York, pp 277–305
Laws ER Jr, Trautmann JC, Hollenhorst RW Jr (1977) Transsphenoidal decompression of the optic nerve and chiasm. Visual results in 62 patients. J Neurosurg 46:717–722
Lennerstrand G (1983) Visual recovery after treatment for pituitary adenoma. Acta Ophthalmol (Copenh) 61:1104–1117
Lewin JS, Nour SG, Meyers ML, Metzger AK, Maciunas RJ, Wendt M, Duerk JL, Oppelt A, Selman WR (2007) Intraoperative MRI with a rotating, tiltable surgical table: a time use study and clinical results in 122 patients. AJR Am J Roentgenol 189:1096–1103
Littley MD, Shalet SM, Beardwell CG, Ahmed SR, Applegate G, Sutton ML (1989) Hypopituitarism following external radiotherapy for pituitary tumours in adults. Q J Med 70:145–160
Losa M, Franzin A, Mangili F, Terreni MR, Barzaghi R, Veglia F, Mortini P, Giovanelli M (2000) Proliferation index of nonfunctioning pituitary adenomas: correlations with clinical characteristics and long-term follow-up results. Neurosurgery 47:1313–1318, discussion 1318–1319
Lundin P, Pedersen F (1992) Volume of pituitary macroadenomas: assessment by MRI. J Comput Assist Tomogr 16:519–528
Marazuela M, Astigarraga B, Vicente A, Estrada J, Cuerda C, Garcia-Uria J, Lucas T (1994) Recovery of visual and endocrine function following transsphenoidal surgery of large nonfunctioning pituitary adenomas. J Endocrinol Invest 17:703–707
Marcus M, Vitale S, Calvert PC, Miller NR (1991) Visual parameters in patients with pituitary adenoma before and after transsphenoidal surgery. Aust N Z J Ophthalmol 19:111–118
Martin CH, Schwartz R, Jolesz F, Black PM (1999) Transsphenoidal resection of pituitary adenomas in an intraoperative MRI unit. Pituitary 2:155–162
McPherson CM, Bohinski RJ, Dagnew E, Warnick RE, Tew JM (2003) Tumor resection in a shared-resource magnetic resonance operating room: experience at the University of Cincinnati. Acta Neurochir Suppl 85:39–44
Meng XH, Xu BN, Wei SB, Zhou T, Chen XL, Yu XG, Zhou DB, Tong HY, Zhang JS, Zhao Y, Hou YZ (2011) High-field intraoperative magnetic resonance imaging suite with neuronavigation system: implementation and preliminary experience in the pituitary adenoma operation with transsphenoidal approach. Zhonghua Wai Ke Za Zhi 49:703–706
Nelson AT Jr, Tucker HS Jr, Becker DP (1984) Residual anterior pituitary function following transsphenoidal resection of pituitary macroadenomas. J Neurosurg 61:577–580
Netuka D, Masopust V, Belsan T, Kramar F, Benes V (2011) One year experience with 3.0 T intraoperative MRI in pituitary surgery. Acta Neurochir Suppl 109:157–159
Nimsky C, Ganslandt O, Fahlbusch R (2004) Functional neuronavigation and intraoperative MRI. Adv Tech Stand Neurosurg 29:229–263
Nimsky C, Ganslandt O, Fahlbusch R (2005) Comparing 0.2 tesla with 1.5 tesla intraoperative magnetic resonance imaging analysis of setup, workflow, and efficiency. Acad Radiol 12:1065–1079
Nimsky C, Ganslandt O, Hofmann B, Fahlbusch R (2003) Limited benefit of intraoperative low-field magnetic resonance imaging in craniopharyngioma surgery. Neurosurgery 53:72–80, discussion 80–71
Nimsky C, Ganslandt O, Von Keller B, Romstock J, Fahlbusch R (2004) Intraoperative high-field-strength MR imaging: implementation and experience in 200 patients. Radiology 233:67–78
Nimsky C, von Keller B, Ganslandt O, Fahlbusch R (2006) Intraoperative high-field magnetic resonance imaging in transsphenoidal surgery of hormonally inactive pituitary macroadenomas. Neurosurgery 59:105–114, discussion 105–114
Noh TW, Jeong HJ, Lee MK, Kim TS, Kim SH, Lee EJ (2009) Predicting recurrence of nonfunctioning pituitary adenomas. J Clin Endocrinol Metab 94:4406–4413
Nomikos P, Ladar C, Fahlbusch R, Buchfelder M (2004) Impact of primary surgery on pituitary function in patients with non-functioning pituitary adenomas – a study on 721 patients. Acta Neurochir (Wien) 146:27–35
Orija IB, Weil RJ, Hamrahian AH (2012) Pituitary incidentaloma. Best Pract Res Clin Endocrinol Metab 26:47–68
Pamir MN (2011) 3 T ioMRI: the Istanbul experience. Acta Neurochir Suppl 109:131–137
Pamir MN, Peker S, Ozek MM, Dincer A (2006) Intraoperative MR imaging: preliminary results with 3 tesla MR system. Acta Neurochir Suppl 98:97–100
Pandin P, Dewitte O (2007) Open low-field intraoperative MRI for transsphenoidal pituitary surgery. Anesth Analg 105:886
Pergolizzi RS Jr, Nabavi A, Schwartz RB, Hsu L, Wong TZ, Martin C, Black PM, Jolesz FA (2001) Intra-operative MR guidance during trans-sphenoidal pituitary resection: preliminary results. J Magn Reson Imaging 13:136–141
Peter M, De Tribolet N (1995) Visual outcome after transsphenoidal surgery for pituitary adenomas. Br J Neurosurg 9:151–157
Powell M (1995) Recovery of vision following transsphenoidal surgery for pituitary adenomas. Br J Neurosurg 9:367–373
Ramirez C, Cheng S, Vargas G, Asa SL, Ezzat S, Gonzalez B, Cabrera L, Guinto G, Mercado M (2012) Expression of Ki-67, PTTG1, FGFR4, and SSTR 2, 3, and 5 in nonfunctioning pituitary adenomas: a high throughput TMA, immunohistochemical study. J Clin Endocrinol Metab 97:1745–1751
Reddy R, Cudlip S, Byrne JV, Karavitaki N, Wass JA (2011) Can we ever stop imaging in surgically treated and radiotherapy-naive patients with non-functioning pituitary adenoma? Eur J Endocrinol 165:739–744
Roelfsema F, Biermasz NR, Pereira AM (2012) Clinical factors involved in the recurrence of pituitary adenomas after surgical remission: a structured review and meta-analysis. Pituitary 15:71–83
Sandeman D, Moufid A (1998) Interactive image-guided pituitary surgery. An experience of 101 procedures. Neurochirurgie 44:331–338
Schulder M, Jacobs A, Carmel PW (2001) Intraoperative MRI and adjuvant radiosurgery. Stereotact Funct Neurosurg 76:151–158
Schwartz TH, Stieg PE, Anand VK (2006) Endoscopic transsphenoidal pituitary surgery with intraoperative magnetic resonance imaging. Neurosurgery 58:ONS44–ONS51, discussion ONS44-51
Sheehan JP, Starke RM, Mathieu D, Young B, Sneed PK, Chiang VL, Lee JY, Kano H, Park KJ, Niranjan A, Kondziolka D, Barnett GH, Rush S, Golfinos JG, Lunsford LD (2013) Gamma Knife radiosurgery for the management of nonfunctioning pituitary adenomas: a multicenter study. J Neurosurg 119:446–456
Shou XF, Li SQ, Wang YF, Zhao Y, Jia PF, Zhou LF (2005) Treatment of pituitary adenomas with a transsphenoidal approach. Neurosurgery 56:249–256, discussion 249–256
Shults WT, Miller NR (1998) Compressive optic neuropathies. In: Miller NR, Newman NJ (eds) Walsh & Hoyt’s Clinical Neuroophthalmology, 5th edn. Williams & Wilkins, Baltimore, pp 657–658
Steinmeier R, Fahlbusch R, Ganslandt O, Nimsky C, Buchfelder M, Kaus M, Heigl T, Lenz G, Kuth R, Huk W (1998) Intraoperative magnetic resonance imaging with the magnetom open scanner: concepts, neurosurgical indications, and procedures: a preliminary report. Neurosurgery 43:739–747, discussion 747–738
Szerlip NJ, Zhang YC, Placantonakis DG, Goldman M, Colevas KB, Rubin DG, Kobylarz EJ, Karimi S, Girotra M, Tabar V (2011) Transsphenoidal resection of sellar tumors using high-field intraoperative magnetic resonance imaging. Skull base : official journal of North American Skull Base Society … [et al.] 21:223–232
Theodosopoulos PV, Leach J, Kerr RG, Zimmer LA, Denny AM, Guthikonda B, Froelich S, Tew JM (2010) Maximizing the extent of tumor resection during transsphenoidal surgery for pituitary macroadenomas: can endoscopy replace intraoperative magnetic resonance imaging? J Neurosurg 112:736–743
Trautmann JC, Laws ER Jr (1983) Visual status after transsphenoidal surgery at the Mayo Clinic, 1971–1982. Am J Ophthalmol 96:200–208
members of H, Trouillas J, Roy P, Sturm N, Dantony E, Cortet-Rudelli C, Viennet G, Bonneville JF, Assaker R, Auger C, Brue T, Cornelius A, Dufour H, Jouanneau E, Francois P, Galland F, Mougel F, Chapuis F, Villeneuve L, Maurage CA, Figarella-Branger D, Raverot G, Barlier A, Bernier M, Bonnet F, Borson-Chazot F, Brassier G, Caulet-Maugendre S, Chabre O, Chanson P, Cottier JF, Delemer B, Delgrange E, Di Tommaso L, Eimer S, Gaillard S, Jan M, Girard JJ, Lapras V, Loiseau H, Passagia JG, Patey M, Penfornis A, Poirier JY, Perrin G, Tabarin A (2013) A new prognostic clinicopathological classification of pituitary adenomas: a multicentric case–control study of 410 patients with 8 years post-operative follow-up. Acta Neuropathol 126:123–135
Walker DG, Ohaegbulam C, Black PM (2002) Frameless stereotaxy as an alternative to fluoroscopy for transsphenoidal surgery: use of the InstaTrak-3000 and a novel headset. J Clin Neurosci 9:294–297
Webb SM, Rigla M, Wagner A, Oliver B, Bartumeus F (1999) Recovery of hypopituitarism after neurosurgical treatment of pituitary adenomas. J Clin Endocrinol Metab 84:3696–3700
Wu JS, Shou XF, Yao CJ, Wang YF, Zhuang DX, Mao Y, Li SQ, Zhou LF (2009) Transsphenoidal pituitary macroadenomas resection guided by PoleStar N20 low-field intraoperative magnetic resonance imaging: comparison with early postoperative high-field magnetic resonance imaging. Neurosurgery 65:63–70, discussion 70–61
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This paper has an important message: residual adenomas from transsphenoidal surgery recur whether a microscope or an endoscope is used, and if one uses an iMRI, there will be fewer residuals in one's personal series, and thus fewer recurrences. Many experienced transsphenoidal surgeons have found the extra time required for iMRI irksome and therefore not worth it. This paper suggests they should try iMRI again.
Michael Powell
London,UK
Rights and permissions
About this article

Cite this article
Berkmann, S., Schlaffer, S., Nimsky, C. et al. Follow-up and long-term outcome of nonfunctioning pituitary adenoma operated by transsphenoidal surgery with intraoperative high-field magnetic resonance imaging. Acta Neurochir 156, 2233–2243 (2014). https://doi.org/10.1007/s00701-014-2210-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-014-2210-x