
Abstract
Background
Eyebrow craniotomy is a recently described minimally invasive approach for tackling primarily pathology of the anterior skull base. The removal of the orbital bar may further expand the surgical corridor of this exposure, but the extent of benefit is poorly quantified. We assessed the effect of orbital bar removal with regards to surgical access in the eyebrow craniotomy using classic morphometric measurements in cadaver heads. Using surgical phantoms and neuronavigation, we also measured the ‘working volume’, a new parameter for characterising the volume of surgical access in these approaches.
Methods
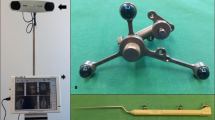
Silicon injected cadaver heads (n = 5) were used for morphometric analysis of the eyebrow craniotomy with and without orbital bar removal. Working depths and ‘working areas’ of surgical access were measured as defined by key anatomical landmarks. The eyebrow craniotomy with or without orbital bar removal was also simulated using surgical phantoms (n = 3, 90–120 points per trial), calibrated against a frameless neuronavigation system. Working volume was derived from reference coordinates recorded along the anatomical borders of the eyebrow craniotomy using the “α-shape algorithm” in R statistics.
Results
In cadaver heads, eyebrow craniotomy with removal of the orbital bar reduced the working depth to the ipsilateral anterior clinoid process (42 ± 2 versus 33 ± 3 mm; p < 0.05), but the working areas as defined by deep neurovascular and bony landmarks was statistically unchanged (total working areas of 418 ± 80 cm2 versus 334 ± 48 cm2; p = 0.4). In surgical phantom studies, however, working-volume for the simulated eyebrow craniotomies was increased with orbital bar removal (16 ± 1 cm3 versus 21 ± 1 cm3; p < 0.01).
Conclusions
In laboratory studies, orbital bar removal in eyebrow craniotomy provides a modest reduction in working depth and increase in the working volume. But this must be weighed up against the added morbidity of the procedure. Working volume, a newly developed parameter may provide a more meaningful endpoint for characterising the surgical access for different surgical approaches and it could be applied to other operative cases undertaken with frameless neuronavigation.




Similar content being viewed by others

References
Beretta F, Andaluz N, Chalaala C, Bernucci C, Salud L, Zuccarello M (2010) Image-guided anatomical and morphometric study of supraorbital and trans-orbital minicraniotomies to the sellar and parasellar regions: comparison with standard techniques. J Neurosurg 113:975–981
Beseoglu K, Lodes S, Stummer W, Steiger HJ, Hänggi DJ (2011) The transorbital keyhole approach: early and long-term outcome analysis of approach-related morbidity and cosmetic results. Tech Note J Neurosurg 114:852–856
Cavalcanti DD, García-González U, Agrawal A, Crawford NR, Tavares PL, Spetzler RF, Preul MC (2010) Quantitative anatomic study of the transcilliary supraorbital approach: benefits of additional orbital osteotomy? Neurosurgery 66:205–210
Cheng CM, Noguchi A, Dogan A, Anderson GJ, Hsu FP, McMenomey SO, Delashaw JB Jr (2013) Quantitative verification of the keyhole concept: a comparison of area of exposure in the parasellar region via supraorbital keyhole, fronto-temporal pterional, and supraorbital approaches. J Neurosurg 118:264–269
D’Ambrosio AL, Mocco J, Hankinson TC, Bruce JN, van Loveren HR (2008) Quantification of the frontotemporal orbitozygomatic approach using a three-dimensional visualization and modeling application. Neurosurgery 62:251–260
Edelsbrunner H, Mucke EP (1994) Three-dimensional alpha shapes. ACM Trans Graph 13:43–72
Figueiredo EG, Deshmukh V, Nakaji P, Deshmukh P, Crusius MU, Crawford N, Spetzler RF, Preul MC (2006) An anatomical evaluation of the mini-supraorbital approach and comparison with standard craniotomies. Neurosurgery 59:ONS212–ONS220
Figueiredo EG, Deshmukh P, Zabramski JM, Preul MC, Crawford NR, Siwanuwatn R, Spetzler RF (2005) Quantitative anatomic study of three surgical approaches to the anterior communicating artery complex. Neurosurgery 56:397–405
Filipce V, Pillai P, Makiese O, Zarzour H, Pigott M, Ammirati M (2009) Quantitative and qualitative analysis of the working area obtained by endoscope and microscope in various approaches to the anterior communicating artery complex using computed tomography-based frameless stereotaxy: a cadaver study. Neurosurgery 65:1147–1152
Frazier CHI (1913) An approach to the hypophysis through the anterior cranial fossa. Ann Surg 57:145–150
Gonzalez LF, Crawford NR, Horgan MA, Deshmukh P, Zabramski JM, Spetzler RF (2002) Working area and angle of attack in three cranial base approaches: pterional, orbitozygomatic, and maxillary extension of the orbitozygomatic approach. Neurosurgery 50:550–555
Horgan MA, Anderson GJ, Kellogg JX, Schwartz MS, Spektor S, McMenomey SO, Delashaw JB (2000) Classification and quantification of the petrosal approach to the petroclival region. J Neurosurg 93:108–112
Krause F (1908) Chirurgie des Gehirns und Rückenmarks nach eigenen Erfahrungen. Urban & Schwarzenberg, Berlin
Perneczky A, Reisch R (2008) Keyhole approaches in neurosurgery, volume 1: concept and surgical technique. Springer, Berlin
Ramos-Zúñiga R (1999) The trans-supraorbital approach. Minim Invasive Neurosurg 42:133–136
Ramos-Zúñiga R, Velázquez H, Barajas MA, López R, Sánchez E, Trejo S (2002) Trans-supraorbital approach to supratentorial aneurysms. Neurosurgery 51:125–130, discussion 130-1
Reisch R, Perneczky A (2005) Ten-year experience with the supraorbital subfrontal approach through an eyebrow skin incision. Neurosurgery 57:242–255
Stadie AT, Kockro RA, Reisch R, Tropine A, Boor S, Stoeter P, Perneczky A (2008) Virtual reality system for planning minimally invasive neurosurgery. Tech Note J Neurosurg 108:382–394
Steiger HJ, Schmid-Elsaesser R, Stummer W, Uhl E (2001) Transorbital keyhole approach to anterior communicating artery aneurysms. Neurosurgery 48:347–351, discussion 351-2
Warren WL, Grant GA (2009) Transcilliary orbitofrontozygomatic approach to lesions of the anterior cranial fossa. Neurosurgery 64:324–329, discussion 329-30
Yasargil GM, Fox JL, Ray MW (1975) Operative approach to aneurysms of the anterior communicating artery. In: Krayenbühl H (ed) Advances and technical standards in neurosurgery, vol 2. Springer, Wein New York, pp 113-170
Zador Z, Gnanalingham K (2013) Eyebrow craniotomy for anterior skull base lesions: how I do it. Acta Neurochir (Wien) 155:99–106
Zador Z, Lu DC, Arnold CM, Lawton MT (2010) Deep bypasses to the distal posterior circulation: anatomical and clinical comparison of pretemporal and subtemporal approaches. Neurosurgery 66:92–100
Acknowledgements
The authors would like to thank Jose Anton-Rodriguez for CT imaging of the skull phantom and Christine Arnold for her work with preparing the cadaver heads.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This cadaver study demonstrated very precisely the advantage and disadvantage of surgical access in eyebrow craniotomy with and without orbital bar removal.
In my opinion the results of this study are important and should be considered before planing surgical approaches.
Daniel Haenggi
Duesseldorf, Germany
Rights and permissions
About this article
Cite this article
Zador, Z., Coope, D.J., Gnanalingham, K. et al. Quantifying surgical access in eyebrow craniotomy with and without orbital bar removal: cadaver and surgical phantom studies. Acta Neurochir 156, 697–702 (2014). https://doi.org/10.1007/s00701-013-1947-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-013-1947-y