
Abstract
Background
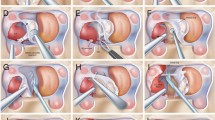
Surgeons undertaking transsphenoidal surgery in patients with acromegaly confront multiple unique challenges secondary to the anatomic alterations caused by growth hormone–secreting tumors. The senior author has noted a fusiform dilatation of the cavernous carotid artery in many acromegalic patients. The authors aim to quantify this dilatation and correlate it with potential contributing factors.
Methods
Clinical and radiographic data were retrospectively assessed in acromegalic patients undergoing transsphenoidal surgery from 2000 through 2011. Randomly selected patients with nonsecreting pituitary adenomas were used as the control cohort. Demographic information, comorbidities, and preoperative growth hormone and insulin-like growth factor-1 levels were recorded. Magnetic resonance (MR) imaging variables included tumor size, diameters of the petrous, cavernous, and supraclinoid segments of the carotid artery, and extent and location of cavernous sinus invasion. Independent correlations between acromegaly and each variable were assessed with multivariate regression analysis.
Results
Forty randomly selected patients with growth hormone–secreting adenomas who underwent surgery and had MR imaging with thin coronal slices of the pituitary region were enlisted in our study cohort. The mean age was 45.7 years. Forty-two males (52.5 %) were included in the study. Mean carotid artery diameter measurements for acromegalic and control patients, respectively, were 4.2 vs. 3.8 mm (petrous carotid), 5.0 vs. 4.0 mm (cavernous carotid), and 3.3 vs. 2.9 mm (supraclinoid carotid). Multivariate analysis showed only age and cavernous carotid diameter were statistically significant independent variables (p = 0.02, p < 0.001, respectively). Age, tumor size, growth-hormone or insulin-like growth factor-1 levels, and cavernous sinus invasion did not correlate with cavernous carotid artery diameter.
Conclusions
In patients with acromegaly, there is a fusiform dilatation of the cavernous carotid artery that must be considered when planning transsphenoidal surgery.



Similar content being viewed by others


References
Colao A, Ferone D, Marzullo P, Lombardi G (2004) Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr Rev 25:102–152
Couldwell WT (2004) Transsphenoidal and transcranial surgery for pituitary adenomas. J Neurooncol 69:237–256
Dougherty TB, Cronau LH Jr (1998) Anesthetic implications for surgical patients with endocrine tumors. Int Anesthesiol Clin 36:31–44
Ebner FH, Kuerschner V, Dietz K, Bueltmann E, Naegele T, Honegger J (2009) Reduced intercarotid artery distance in acromegaly: pathophysiologic considerations and implications for transsphenoidal surgery. Surg Neurol 72:456–460, discussion 460
Harris AG (1996) Acromegaly and its managment. Lippincott-Raven Publishers, Philadephia
Laws ER (2008) Surgery for acromegaly: evolution of the techniques and outcomes. Rev Endocr Metab Disord 9:67–70
Laws ER Jr (1999) Vascular complications of transsphenoidal surgery. Pituitary 2:163–170
Laws ER Jr, Piepgras DG, Randall RV, Abboud CF (1979) Neurosurgical management of acromegaly. Results in 82 patients treated between 1972 and 1977. J Neurosurg 50:454–461
Liu JK, Weiss MH, Couldwell WT (2003) Surgical approaches to pituitary tumors. Neurosurg Clin N Am 14:93–107
Manara R, Maffei P, Citton V, Rizzati S, Bommarito G, Ermani M, Albano I, Della Puppa A, Carollo C, Pavesi G, Scanarini M, Ceccato F, Sicolo N, Mantero F, Scaroni C, Martini C (2011) Increased rate of intracranial saccular aneurysms in acromegaly: an MR angiography study and review of the literature. J Clin Endocrinol Metab 96:1292–1300
Nemergut EC, Dumont AS, Barry UT, Laws ER (2005) Perioperative management of patients undergoing transsphenoidal pituitary surgery. Anesth Analg 101:1170–1181
Oshino S, Nishino A, Suzuki T, Arita H, Tateishi A, Matsumoto K, Shimokawa T, Kinoshita M, Yoshimine T, Saitoh Y (2012) Prevalence of cerebral aneurysm in patients with acromegaly. Pituitary. doi:10.1007/s11102-012-0404-x
Saeki N, Iuchi T, Higuchi Y, Uchino Y, Murai H, Isono S, Yasuda T, Minagawa M, Yamaura A, Sunami K (2000) Bone CT evaluation of nasal cavity of acromegalics—its morphological and surgical implication in comparison to non-acromegalics. Endocr J 47(Suppl):S65–S68
Sivakumar W, Chamoun R, Nguyen V, Couldwell WT (2011) Incidental pituitary adenomas. Neurosurg Focus 31(6):E18
Skinner DW, Richards SH (1988) Acromegaly—the mucosal changes within the nose and paranasal sinuses. J Laryngol Otol 102:1107–1110
van der Lely AJ, Beckers A, Daly AF, Lamberts SW, Clemmons DR (2005) Acromegaly—pathology, diagnosis, and treatment. Taylor & Francis Group, Boca Raton
Weir B (1992) Pituitary tumors and aneurysms: case report and review of the literature. Neurosurgery 30:585–591
White PM, Wardlaw JM (2003) Unruptured intracranial aneurysms. J Neuroradiol 30:336–350
Zada G, Cavallo LM, Esposito F, Fernandez-Jimenez JC, Tasiou A, De Angelis M, Cafiero T, Cappabianca P, Laws ER (2010) Transsphenoidal surgery in patients with acromegaly: operative strategies for overcoming technically challenging anatomical variations. Neurosurg Focus 29(4):E8
Zada G, Sivakumar W, Fishback D, Singer PA, Weiss MH (2010) Significance of postoperative fluid diuresis in patients undergoing transsphenoidal surgery for growth hormone-secreting pituitary adenomas. J Neurosurg 112:744–749
Acknowledgments
The authors thank Kristin Kraus, M.Sc., for her steadfast assistance in the preparation of this article and Jennie Swensen, M.A., for her medical illustration.
Conflicts of interest
None.
Author contribution
Conception and design: Couldwell, Chamoun, Sivakumar. Acquisition of data: Chamoun, Salzman, Sivakumar. Analysis and interpretation of data: Couldwell, Riva-Cambrin, Chamoun, Sivakumar. Drafting the article: Sivakumar. Critically revising the article: all authors. Reviewed submitted version of the manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Couldwell. Statistical analysis: Riva-Cambrin, Sivakumar. Study supervision: Couldwell.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This is an interesting paper, but of course without a conclusion as to why these tumours should cause dilatation. I was frankly surprised that neither hypertension nor, particularly, diabetes was more prevalent as our acromegalics are definitely more often diabetic and, I thought, hypertensive. Perhaps this is a phenomenon of healthy Utah.
I would be interested if this same study could be done on your Cushing's patients, which I understand is in preparation. Perhaps this will give the answer.
The message—surgeon beware the carotid in acromegalics—is a useful reminder.
Michael Powell
London, UK
Rights and permissions
About this article
Cite this article
Sivakumar, W., Chamoun, R.B., Riva-Cambrin, J. et al. Fusiform dilatation of the cavernous carotid artery in acromegalic patients. Acta Neurochir 155, 1077–1083 (2013). https://doi.org/10.1007/s00701-013-1691-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-013-1691-3