
Abstract
Background
Adrenal insufficiency is a feared complication in patients undergoing transphenoidal surgery (TSS). Using the insulin tolerance test (ITT) for the preoperative assessment of hypothalamic-pituitary-adrenal (HPA) status is less than ideal, and the morning serum cortisol (MSC) is often used as a proxy for ITT. However, neither the ITT nor the MSC level has been validated to indicate HPA sufficiency compared to a physiological gold standard such as patients’ ability to withstand transphenoidal surgery.
Objective
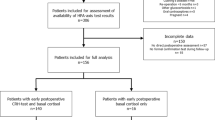
To evaluate the intraoperative and postoperative course of nine patients with non-ACTH-secreting pituitary adenomas who did not receive intraoperative cortisol replacement despite having a preoperative MSC below 9 μg/dl (250 nmol/l) and to compare this with a set of patients with a preoperative MSC greater than 14.5 μg/dl (400 nmol/l) and another set of patients with MSC below 9 μg/dl (250 nmol/l) who received intraoperative cortisol administration.
Methods
Preoperative and day 1 and day 2 postoperative MSC, intraoperative anesthetic record, vital signs, fluid balance, medications, and complications were recorded.
Results
None of the patients experienced the full syndrome of adrenal insufficiency. One patient with a preoperative MSC <9 μg/dl (250 mol/l) had isolated postoperative fatigue and required cortisol replacement. No patient suffered any life-threatening complications. There were no differences among the three groups in their intraoperative or postoperative courses when compared for intraoperative hypotension, acute blood pressure drop, and administration of vasopressors.
Conclusion
This study suggests that TSS can be performed safely in patients with preoperative MSC less than 9 μg/dl (250 nmol/l) in closely monitored settings without intraoperative cortisol administration. Further studies are warranted.

Similar content being viewed by others


References
Fraser CG, Preuss FS, Bigford WD (1952) Adrenal atrophy and irreversible shock associated with cortisone therapy. J Am Med Assoc 149:1542–1543
Lewis L, Robinson RF, Yee J, Hacker LA, Eisen G (1953) Fatal adrenal cortical insufficiency precipitated by surgery during prolonged continuous cortisone treatment. Ann Intern Med 39:116–126
Auchus RJ, Shewbridge RK, Shepherd MD (1997) Which patients benefit from provocative adrenal testing after transsphenoidal pituitary surgery? Clin Endocrinol (Oxf) 46:21–27
Marko NF, Gonugunta VA, Hamrahian AH, Usmani A, Mayberg MR, Weil RJ (2009) Use of morning serum cortisol level after transsphenoidal resection of pituitary adenoma to predict the need for long-term glucocorticoid supplementation. J Neurosurg 111:540–544
Rajasekaran S, Vanderpump M, Baldeweg S, Drake W, Reddy N, Lanyon M, Markey A, Plant G, Powell M, Sinha S, Wass J (2011) UK guidelines for the management of pituitary apoplexy. Clin Endocrinol 74:9–20
Salem M, Tainsh RE Jr, Bromberg J, Loriaux DL, Chernow B (1994) Perioperative glucocorticoid coverage. A reassessment 42 years after emergence of a problem. Ann Surg 219:416–425
Fish HR, Chernow B, O’Brian JT (1986) Endocrine and neurophysiologic responses of the pituitary to insulin-induced hypoglycemia: a review. Metabolism 35:763–780
Karaca Z, Tanriverdi F, Atmaca H, Gokce C, Elbuken G, Selcuklu A, Unluhizarci K, Kelestimur F (2010) Can basal cortisol measurement be an alternative to the insulin tolerance test in the assessment of the hypothalamic-pituitary-adrenal axis before and after pituitary surgery? Eur J Endocrinol 163:377–382
Plumpton FS, Besser GM (1969) The adrenocortical response to surgery and insulin-induced hypoglycaemia in corticosteroid-treated and normal subjects. Br J Surg 56:216–219
Pfeifer M, Kanc K, Verhovec R, Kocijancic A (2001) Reproducibility of the insulin tolerance test (ITT) for assessment of growth hormone and cortisol secretion in normal and hypopituitary adult men. Clin Endocrinol (Oxf) 54:17–22
Bhansali A, Dutta P, Bhat MH, Mukherjee KK, Rajput R, Bhadada S (2008) Rational use of glucocorticoid during pituitary surgery–a pilot study. Indian J Med Res 128:294–299
Hagg E, Asplund K, Lithner F (1987) Value of basal plasma cortisol assays in the assessment of pituitary-adrenal insufficiency. Clin Endocrinol (Oxf) 26:221–226
Jayasena CN, Gadhvi KA, Gohel B, Martin NM, Mendoza N, Meeran K, Dhillo WS (2009) Day 5 morning serum cortisol predicts hypothalamic-pituitary-adrenal function after transsphenoidal surgery for pituitary tumors. Clin Chem 55:972–977
Abdu TA, Elhadd TA, Neary R, Clayton RN (1999) Comparison of the low dose short synacthen test (1 microg), the conventional dose short synacthen test (250 microg), and the insulin tolerance test for assessment of the hypothalamo-pituitary-adrenal axis in patients with pituitary disease. J Clin Endocrinol Metab 84:838–843
Cozzi R, Lasio G, Cardia A, Felisati G, Montini M, Attanasio R (2009) Perioperative cortisol can predict hypothalamus-pituitary-adrenal status in clinically non-functioning pituitary adenomas. J Endocrinol Invest 32:460–464
Avgerinos PC, Schurmeyer TH, Gold PW, Tomai TP, Loriaux DL, Sherins RJ, Cutler GB Jr, Chrousos GP (1986) Pulsatile administration of human corticotropin-releasing hormone in patients with secondary adrenal insufficiency: restoration of the normal cortisol secretory pattern. J Clin Endocrinol Metab 62:816–821
Kehlet (1976) Clinical course and hypothalamic-pituitary-adreno-cortical function in glucocorticoid-treated surgical patients. FADL’s Forlag, Copenhagen
Masala A, Satta G, Alagna S, Anania V, Frassetto GA, Rovasio PP, Semiani A (1985) Effect of clonidine on stress-induced cortisol release in man during surgery. Pharmacol Res Commun 17:293–298
Reincke M, Allolio B, Wurth G, Winkelmann W (1993) The hypothalamic-pituitary-adrenal axis in critical illness: response to dexamethasone and corticotropin-releasing hormone. J Clin Endocrinol Metab 77:151–156
Schlaghecke R, Kornely E, Santen RT, Ridderskamp P (1992) The effect of long-term glucocorticoid therapy on pituitary-adrenal responses to exogenous corticotropin-releasing hormone. N Engl J Med 326:226–230
Wand GS, Ney RL (1985) Disorders of the hypothalamic-pituitary-adrenal axis. Clin Endocrinol Metab 14:33–53
Mathes DD, Assimos DG, Donofrio PD (1996) Rhabdomyolysis and myonecrosis in a patient in the lateral decubitus position. Anesthesiology 84:727–729
Chernow B, Alexander HR, Smallridge RC, Thompson WR, Cook D, Beardsley D, Fink MP, Lake CR, Fletcher JR (1987) Hormonal responses to graded surgical stress. Arch Intern Med 147:1273–1278
Carey LC, Lowery BD, Cloutier CT (1970) Blood sugar and insulin response of humans in shock. Ann Surg 172:342–350
Nieman LK (2009) ACTH and cortisol secretion in health and disease.
Carey LC, Cloutier CT, Lowery BD (1971) Growth hormone and adrenal cortical response to shock and trauma in the human. Ann Surg 174:451–460
Meguid MM, Brennan MF, Aoki TT, Muller WA, Ball MR, Moore FD (1974) Hormone-substrate interrelationships following trauma. Arch Surg 109:776–783
Udelsman R, Goldstein DS, Loriaux DL, Chrousos GP (1987) Catecholamine-glucocorticoid interactions during surgical stress. J Surg Res 43:539–545
Udelsman R, Ramp J, Gallucci WT, Gordon A, Lipford E, Norton JA, Loriaux DL, Chrousos GP (1986) Adaptation during surgical stress. A reevaluation of the role of glucocorticoids. J Clin Invest 77:1377–1381
Aizawa T, Yasuda N, Greer MA (1981) Hypoglycemia stimulates ACTH secretion through a direct effect on the basal hypothalamus. Metabolism 30:996–1000
Udelsman R, Norton JA, Jelenich SE, Goldstein DS, Linehan WM, Loriaux DL, Chrousos GP (1987) Responses of the hypothalamic-pituitary-adrenal and renin-angiotensin axes and the sympathetic system during controlled surgical and anesthetic stress. J Clin Endocrinol Metab 64:986–994
Alford WC Jr, Meador CK, Mihalevich J, Burrus GR, Glassford DM Jr, Stoney SW, Thomas CS Jr (1979) Acute adrenal insufficiency following cardiac surgical procedures. J Thorac Cardiovasc Surg 78:489–493
Mohler JL, Michael KA, Freedman AM, McRoberts JW, Griffen WO Jr (1985) The evaluation of postoperative function of the adrenal gland. Surg Gynecol Obstet 161:551–556
Christy NP (1992) Pituitary-adrenal function during corticosteroid therapy. Learning to live with uncertainty. N Engl J Med 326:266–267
Glowniak JV, Loriaux DL (1997) A double-blind study of perioperative steroid requirements in secondary adrenal insufficiency. Surgery 121:123–129
Fraser RAF, Smith PH (1941) The value of the glucose tolerance test, the insulin tolerance test, and the glucose-insulin tolerance test in the diagnosis of endocrinologic disorders of glucose metabolism. J Clin Endocrinol Metab 1:297–306
Schaffranietz L, Wolfel H, Fritz H, Rudolph C (2003) Is the combination of remifentanil and propopfol suitable for transsphenoid resection of the hypophysis? Anaesthesiol Reanim 28:45–49
Liddle GW (1981) The adrenals. In: Williams RH (ed). Textbook of Endocrinology, 6th ed. W.B. Saunders & Co. Philadelphia, pp 249–292
Kehlet H (1975) A rational approach to dosage and preparation of parenteral glucocorticoid substitution therapy during surgical procedures. A short review. Acta Anaesthesiol Scand 19:260–264
Disclosures
I certify that this manuscript was written by myself, Claudio De Tommasi, together with Dr. Michael Cusimano and Dr. Jeannette Goguen. The article was written in adherence with strict ethical rules. No notifications of conflict of interest or financial disclosures have to be made.
Conflict of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
De Tommasi, C., Goguen, J. & Cusimano, M.D. Transphenoidal surgery without steroid replacement in patients with morning serum cortisol below 9 μg/dl (250 Nmol/l). Acta Neurochir 154, 1903–1915 (2012). https://doi.org/10.1007/s00701-012-1474-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-012-1474-2