
Abstract
Background
Although the microvascular decompression (MVD) has become a definitive treatment for the primary hemifacial spasm (HFS), there still are some failed cases. To obtain a satisfactory postoperative outcome, those failure cases of MVD need to be analyzed.
Method
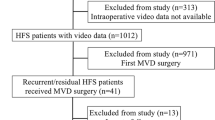
Between January and October 2009, 393 patients with primary HFS underwent MVD. Postoperatively, 375 presented complete spasm-free, 7 improved apparently, and 11 without any improvement at all. A reoperation was performed in 9 of the 11 patients who had poor outcome within 5 days. Those redo MVD cases were reviewed.
Findings
After the reoperation, the symptom of those patients all disappeared immediately. Therefore, the final outcomes were excellent in 97.7%, good in 1.8%, and poor in 0.5%. Up to the 1 year follow-up period, neither recurrence nor change was found. For the two patients without reoperation, their symptoms remained. The previous surgery was a failure due to insufficient decompression in two and conflict missed in seven.
Conclusions
A successful MVD operation is attributable to a thorough exploration of the entire nerve course. An early relief should become the ambition of the operator while performing MVD.


Similar content being viewed by others


References
Campos-Benitez M, Kaufmann AM (2008) Neurovascular compression findings in hemifacial spasm. J Neurosurg 109:416–420
Goto Y, Matsushima T, Natori Y, Inamura T, Tobimatsu S (2002) Delayed effects of the microvascular decompression on hemifacial spasm: a retrospective study of 131 consecutive operated cases. Neurol Res 24:296–300
Hyun SJ, Kong DS, Park K (2010) Microvascular decompression for treating hemifacial spasm: lessons learned from a prospective study of 1,174 operations. Neurosurg Rev 33:325–334, discussion 334
Ishikawa M, Nakanishi T, Takamiya Y, Namiki J (2001) Delayed resolution of residual hemifacial spasm after microvascular decompression operations. Neurosurgery 49:847–854, discussion 854–846
Jannetta PJ, McLaughlin MR, Casey KF (2005) Technique of microvascular decompression. Technical note. Neurosurg Focus 18:E5
Jeon CJ, Kong DS, Lee JA, Park K (2010) The efficacy and safety of microvascular decompression for hemifacial spasm in elderly patients. J Korean Neurosurg Soc 47:442–445
Kim JP, Park BJ, Choi SK, Rhee BA, Lim YJ (2008) Microvascular decompression for hemifacial spasm associated with vertebrobasilar artery. J Korean Neurosurg Soc 44:131–135
Kim HR, Rhee DJ, Kong DS, Park K (2009) Prognostic factors of hemifacial spasm after microvascular decompression. J Korean Neurosurg Soc 45:336–340
Li CS (2005) Varied patterns of postoperative course of disappearance of hemifacial spasm after microvascular decompression. Acta Neurochir (Wien) 147:617–620, discussion 620
McLaughlin MR, Jannetta PJ, Clyde BL, Subach BR, Comey CH, Resnick DK (1999) Microvascular decompression of cranial nerves: lessons learned after 4400 operations. J Neurosurg 90:1–8
Oh ET, Kim E, Hyun DK, Yoon SH, Park H, Park HC (2008) Time course of symptom disappearance after microvascular decompression for hemifacial spasm. J Korean Neurosurg Soc 44:245–248
Park JS, Kong DS, Lee JA, Park K (2008) Chronologic analysis of symptomatic change following microvascular decompression for hemifacial spasm: value for predicting midterm outcome. Neurosurg Rev 31:413–418, discussion 418–419
Perlmutter DH, Petraglia AL, Barbano R, Schwalb JM (2010) Microvascular decompression in patient with atypical features of hemifacial spasm secondary to compression by a tortuous vertebrobasilar system: case report. Neurosurgery 66:E1212, discussion E1212
Sekula RF Jr, Frederickson AM, Jannetta PJ, Bhatia S, Quigley MR (2010) Microvascular decompression after failed gamma knife surgery for trigeminal neuralgia: a safe and effective rescue therapy? J Neurosurg 113:45–52
Sindou M (2009) Trigeminal neuralgia: a plea for microvascular decompression as the first surgical option. Anatomy should prevail. Acta Neurochir (Wien) 152:361–364
Sindou M, Keravel Y (2009) Neurosurgical treatment of primary hemifacial spasm with microvascular decompression. Neurochirurgie 55:236–247
Yuan Y, Wang Y, Zhang SX, Zhang L, Li R, Guo J (2005) Microvascular decompression in patients with hemifacial spasm: report of 1200 cases. Chin Med J (Engl) 118:833–836
Zhong J, Li ST, Xu SQ, Wan L, Wang X (2008) Management of petrosal veins during microvascular decompression for trigeminal neuralgia. Neurol Res 30:697–700
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This paper reports the practical experience of a very experienced team on MVD for primary Hemi Facial-Spasm (HFS). The authors advocate immediate reoperation after failed MVD. The strong belief of the authors is that disappearance of spasms must be obtained as soon as surgery is completed, and if not, that the patient should have re-exploration the first few days after initial surgery. The authors provide arguments for defending this attitude.
Our experience, as well as the one from other, quoted in this article, is far from to be the same as the Shanghai group’s experience. In our past published series of 147 patients followed over more than 1 year and up to 20 years (7 years on average), the long-term cure rate (=total disappearance of symptoms, confirmed by post-op facial EMG, i. e., an excellent result) was of 75%. In addition other 12% had good outcome (=no disabling symptoms in the practical daily life, in spite of some remaining occasional spasms on emotional events). Important to say 13% in the group of patients with excellent or good outcome had a delayed cure of 3 months to 1 year (three for 3 years long). Even more, most of our patients had some remaining facial muscular twitches during the first week after surgery!
Our surgery consisted of:
1. infero-lateral floccular approach of brainstem in between lower cranial nerves (IX–X) caudally and VII–VIII complex rostrally,
2. complete exposure of the facial nerve from ponto-medullary sulcus to meatus,
3. total freeing of the root from arachnoïdal adhesions,
4. dissection/separation of the compressive vessels (several in 35% of patients), excepted the one(s) entering the auditory maetus,
5. transposition of the conflicting vessels and their maintain away with Teflon material not touching the nerve [Sindou M. Keravel Y. (2009) Neurosurgical treatment of primary hemifacial spasm with microvascular decompression. Neurochirurgie 55: 236–247]
Delay in cure can be explained: 1) by little (if not always absence of) surgical manipulations of the facial nerve while doing decompression, 2) by the care taken with the inserted material to maintain the conflicting vessel(s) apart (a small piece of Teflon plate) not to compress, even if possible not to touch at all the facial nerve. This hypothesis is consistent with the putative pathophysiological mechanisms of primary HFS. According to Moller [Moller A. (1999). Vascular compression of cranial nerves. Pathophysiology. Neurol. Resarch 21: 439–443], primary HFS would be due to hyperactivity of the facial nucleus, progressively induced by the chronic compression pulsation of the neuro-vascular conflict, especially at REZ. Thus it would be physiologically logical that the effect of surgical decompression take time to decrease and normalize. The immediate effect of MVD by the Shanghai team might be linked, not only to a very well-performed decompression, but also to a certain degree of “neo-compression” of the facial nerve by the interposed Teflon ball / pledget. This neocompressive effect might generate an at least mild and transient conduction block.
We however agree with professor Zhong that early re-operation could be indicated when attacks of spasms are not significantly alleviated before the planned discharge, but in very specific situations. The first one would be if the entire root was not completely explored due to some (anatomic?) dangerous reasons, for the search of a missed other compressive vessel (in 35% of our cases, several vessels, almost always arteries, contributed to the disease). The second one would be if a potentially offending artery was left in place, especially at the porus of the interval auditory canal, because it was estimated risky to mobilize and transpose it for the hearing function.
We do not think there is a reliable mean to ascertain the completeness of decompression, with the exception of complete checking of the facial root from brainstem to meatus. To be mentioned, after a 3 year experience we abandoned intraoperative EMG monitoring of Lateral spread motor responses, due to practical lack of reliability [Sindou M. (2005) Microsurgical decompression for primary hemifacial spasms. Importance of intraoperative neurophysiological monitoring. Acta Neurochirurgica 147: 1019–1026]
For concluding, excepted in very limited circumstances, we strongly advise to wait, in the order of 1 year after initial surgery, before taking decision for reoperation.
Marc SINDOU
Lyon, France
Rights and permissions
About this article
Cite this article
Zhong, J., Zhu, J., Li, ST. et al. An analysis of failed microvascular decompression in patients with hemifacial spasm: focused on the early reoperative findings. Acta Neurochir 152, 2119–2123 (2010). https://doi.org/10.1007/s00701-010-0794-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-010-0794-3