
Abstract
Introduction
The optimal time point for surgery of intramedullary spinal astrocytomas and ependymomas is often debated on, as predicting factors are poorly defined. The current single-institutional study was conducted to retrospectively analyze prognostic factors for postoperative functional outcome in these patients.
Material and methods
All consecutive adult patients with intramedullary astrocytomas or ependymomas (except filum terminale ependymomas) were included. Imaging data, McCormick score (MCS), and detailed neurological evaluation were stringently applied preoperatively, 1 week, and 6 months postoperatively for functional evaluation of all patients. End points were early and late functional outcome. Prognostic factors were obtained from univariate and multivariate logistic regression analysis.
Results
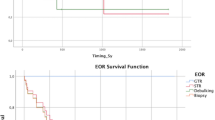
Forty-four patients were included (29 ependymomas World Health Organization (WHO) grades I or II, 8 astrocytomas WHO grade I, and 7 astrocytomas WHO grade II). Overall perioperative morbidity was 34%, and there was no mortality. Complete tumor resection was achieved in 79% of ependymomas, 50% of astrocytomas WHO grade I, and 14% of astrocytomas WHO grade II (significantly more often in ependymomas than in astrocytomas, p < 0.05). Early and late functional outcome were highly intercorrelated (p < 0.01), but not correlated to histology. Preoperative MCS <3 and extent of tumor <5 levels were significantly (p = 0.01 and p < 0.05) associated with a favorable outcome (MCS <3) in early and late follow-up.
Conclusion
An MCS of less than 3 and a tumor extent of less than 5 levels are the most important factors for a favorable postoperative functional outcome. Therefore, surgery should be initiated before significant clinical symptomatology or substantial tumor growth occurs.

Similar content being viewed by others


References
Bowers DC, Weprin BE (2003) Intramedullary spinal cord tumors. Curr Treat Options Neurol 5:207–212
Helseth A, Mork SJ (1989) Primary intraspinal neoplasms in Norway, 1955 to 1986. A population-based survey of 467 patients. J Neurosurg 71:842–845
Epstein FJ, Farmer JP, Freed D (1992) Adult intramedullary astrocytomas of the spinal cord. J Neurosurg 77:355–359
Chang UK, Choe WJ, Chung SK, Chung CK, Kim HJ (2002) Surgical outcome and prognostic factors of spinal intramedullary ependymomas in adults. J Neurooncol 57:133–139
Jenkinson MD, Simpson C, Nicholas RS, Miles J, Findlay DF, Pigott TJ (2006) Outcome predictors and complications in the management of intradural spinal tumors. Eur Spine J 15:203–210
Woodworth GF, Chaichana KL, McGirt MJ, Sciubba DM, Jallo GI, Gokaslan Z, Wolinsky JP, Witham TF (2007) Predictors of ambulatory function after surgical resection of intramedullary spinal cord tumors. Neurosurgery 61:99–105
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, Scheithauer BW, Kleihues P (2007) The 2007 WHO classification of tumors of the central nervous system. Acta Neuropathol 114:97–109
McCormick PC, Torres R, Post KD, Stein BM (1990) Intramedullary ependymoma of the spinal cord. J Neurosurg 72:523–532
Cristante L, Herrmann HD (1994) Surgical management of intramedullary spinal cord tumors: functional outcome and sources of morbidity. Neurosurgery 35:69–74
Hanbali F, Fourney DR, Marmor E, Suki D, Rhines LD, Weinberg JS, McCutcheon IE, Suk I, Gokaslan ZL (2002) Spinal cord ependymoma: radical surgical resection and outcome. Neurosurgery 51:1162–1172
Abul-Kasim K, Thurnher MM, McKeever P, Sundgren PC (2008) Intradural spinal tumors: current classification and MRI features. Neuroradiology 50:301–314, Epub 2007 Dec 15
Bloomer CW, Ackerman A, Bhatia RG (2006) Imaging for spine tumors and new applications. Top Magn Reson Imaging 17:69–87
Brotchi J, Dewitte O, Levivier M, Balériaux D, Vandesteene A, Raftopoulos C, Flament-Durand J, Noterman J (1991) A survey of 65 tumors within the spinal cord: surgical results and the importance of preoperative magnetic resonance imaging. Neurosurgery 29:651–656
Zileli M, Coskun E, Ozdamar N, Ovül I, Tuncbay E, Oner K, Oktar N (1996) Surgery of intramedullary spinal cord tumors. Eur Spine J 5:243–250
Brotchi J, Bruneau M, Lefranc F, Balériaux D (2006) Surgery of intraspinal cord tumors. Clin Neurosurg 53:209–216
Raco A, Esposito V, Lenzi J, Piccirilli M, Delfini R, Cantore G (2005) Long-term follow-up of intramedullary spinal cord tumors: a series of 202 cases. Neurosurgery 56:972–981
Shrivastava RK, Epstein FJ, Perin NI, Post KD, Jallo GI (2005) Intramedullary spinal cord tumors in patients older than 50 years of age: management and outcome analysis. J Neurosurg Spine 2:249–255
Epstein FJ, Farmer JP, Freed D (1993) Adult intramedullary spinal cord ependymomas: the result of surgery in 38 patients. J Neurosurg 79:204–209
Samii M, Klekamp J (1994) Surgical results of 100 intramedullary tumors in relation to accompanying syringomyelia. Neurosurgery 35:865–873
Schwartz TH, McCormick PC (2000) Intramedullary ependymomas: clinical presentation, surgical treatment strategies and prognosis. J Neurooncol 47:211–218
Houten JK, Cooper PR (2000) Spinal cord astrocytomas: presentation, management and outcome. J Neurooncol 47:219–224
Hoshimaru M, Koyama T, Hashimoto N, Kikuchi H (1999) Results of microsurgical treatment for intramedullary spinal cord ependymomas: analysis of 36 cases. Neurosurgery 44:264–269
Adams CBT (1991) Failure of cervical laminectomy to relieve symptoms of cervical myelopathy: an alternative biomechanical view. In: Tarlov EC (ed) Complications of spinal surgery. AANS, Park Ridge, pp 95–104
Wiedemayer H, Sandalcioglu IE, Aalders M, Wiedemayer H, Floerke M, Stolke D (2004) Reconstruction of the laminar roof with miniplates for a posterior approach in intraspinal surgery: technical considerations and critical evaluation of follow-up results. Spine 29:E333–E342
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
This article conveys important information. Despite the fact that surgery is doubtless the best treatment strategy for the tumors included in this series (ependymomas and astrocytomas both pylocitic and diffuse), there is still some argument regarding when it should be recommended. The discussion is certainly more pertinent in cases of incidental tumor finding or in minimally symptomatic patients.
The prevailing idea is that tumor excision should be undertaken at the time of diagnosis. This is based on the fact that not only is surgery the only potentially curative treatment but also because adjuvant treatment plans seem to add little to the arrest or regression of the disease.
This study adds support to the recommendation for early surgery, the authors having found that patients fare better after surgery when lesser extension of the cord is involved by the tumor, and the patient’s preoperative functional level is more favorable.
Interestingly, duration of symptoms did not correlate with tumor type or with preoperative functional status and postoperative outcome. As the authors point out, this only stresses the importance of an early intervention.
Manuel Cunha e Sá, M.D.
Department of Neurosurgery, Hospital Garcia de Orta
Almada, Portugal
Rights and permissions
About this article
Cite this article
Eroes, C.A., Zausinger, S., Kreth, FW. et al. Intramedullary low grade astrocytoma and ependymoma. Surgical results and predicting factors for clinical outcome. Acta Neurochir 152, 611–618 (2010). https://doi.org/10.1007/s00701-009-0577-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-009-0577-x