
Abstract
Background
Evolving of a single centre by means of different transsphenoidal approaches during the survey of methodological advances in pituitary surgery is presented.
Materials and methods
Ninety-three consecutive patients with pituitary adenomas underwent transphenoidal pituitary operations at Gulhane Military Medical Academy from January 1996 to October 2007. Retrospective chart-based analysis of the surgical methods of transsphenoidal pituitary adenoma operations were done. Surgical methods were described. Outcomes and complications were presented. Attention is focused on the methodology of different surgical techniques of pituitary surgery.
Findings
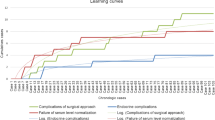
During the evaluation period, 12 Sublabial approaches (1996–1998), 13 transseptal transsphenoidal approaches (1999–2000), 15 endonasal transsphenoidal approaches (2000–2004), 25 endoscopy assisted endonasal approaches (2002–2006) and 28 pure endoscopic endonasal approaches (2006–2007) were performed.
Conclusions
Technologic advancements in endoscopy and gaining experience in pituitary surgery drives neurosurgeons toward less invasive approaches.


Similar content being viewed by others


References
Black PMcL, Zervas NT, Candia G (1987) Incidence and management of complications of transsphenoidal operation for pituitary adenomas. Neurosurgery 209:20–924
Cappabianca P, Cavallo LM, Colao A, Del Basso De Caro M, Esposito F, Cirillo S, Lombardi G, de Divitiis E (2002) Endoscopic endonasal transsphenoidal approach: outcome analysis of 100 consecutive procedures. Minim Invasive Neurosurg 45(4):193–200
Charalampaki P, Reisch R, Ayad A, Conrad J, Welschehold S, Perneczky A, Wuster C (2007) Endoscopic endonasal pituitary surgery: surgical and outcome analysis of 50 cases. J Clin Neurosci. 14(5):410–415
Ciric I, Ragin A, Baumgartner C, Pierce D (1997) Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience. Neurosurgery 40:225–237
Couldwell WT (2004) Transsphenoidal and transcranial surgery for pituitary adenomas. Journal of Neuro-Oncology 69:237–256
Dickman JD, Beyer M, Hess BJ (2000) Three-dimensional organization of vestibular related eye movements to rotational motion in pigeons. Vision Res. 40(20):2831–2844
Hardy J (1967) La chirugie de l’hypophyse par voie transsphenoidale. Union Med Can 96:702–712
Jho HD, Carrau RL, Ko Y, Daly MA (1997) Endoscopic pituitary surgery: an early experience. Surg Neurol 47:213–222
Jho HD, Carrau RL (1997) Endoscopic endonasal transsphenoidal surgery: experience with 50 patients. J Neurosurg 87(1):44–51
Kabil MS, Eby JB, Shahinian HK (2005) Fully endoscopic endonasal vs. transseptal transsphenoidal pituitary surgery. Minim Invasive Neurosurg 48(6):348–354
Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R (2005) Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 15(1):19
Koc K, Anik I, Ozdamar D, Cabuk B, Keskin G, Ceylan S (2006) The learning curve in endoscopic pituitary surgery and our experience. Neurosurg Rev 29:298–305
Laws ER Jr, Piepgras DG, Randall RV, Abboud CF (1979) Neurosurgical management of acromegaly. Results in 82 patients treated between 1972 and 1977. J Neurosurg 50:454–461
Laws ER Jr (1987) Pituitary surgery. Endocrinol Metab Clin N Am 16:647–665
Liu JK, Das K, Weiss MH, Laws ER Jr, Couldwell WT (2001) The history and evolution of transsphenoidal surgery. J Neurosurg 95(6):1083–1096
Rhoton AL (2002) The sellar region. Neurosurgery 51(Suppl 1):335–374
Spencer WR, Das K, Nwagwu C, Wenke E, Schaeffer SD, Moscatello A, Couldwell WT (1999) Approaches to the sellar and parasellar region: anatomic comparison of the microscope vs endoscope. Laryngoscope 109:791–794
Youssef AS, Agazzi S, van Loveren HR (2005) Transcranial surgery for pituitary adenomas. Neurosurgery 571(Suppl):168–175
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This paper provides a longitudinal view of the progression in technique for surgery of pituitary lesions over the past decade or so. This period was marked by increasing enthusiasm for the trans-nasal endoscopic approach, and by the adoption of this technique by several forward-looking groups in many parts of the world.
Along with others, the investigators began with the traditional sub-labial microscopic approach which has served patients so well for many years after its re-introduction in the 1970’s. Along with others, they then moved to the direct endo-nasal microscopic approach which has been considered quicker and less “invasive”. The next step was the introduction of the endoscope in traditional endo-nasal exposures, using the nasal speculum or retractor. Finally, they adopted and report upon the “pure” endoscopic approach, without speculum. They also have generally abandoned the use of intraoperative fluoroscopy and neuronavigation. Although their experience is somewhat limited in numbers of patients, the progression is logical and the results are very good.
One of the alleged advantages of the pure endoscopic approach is that it is “minimally invasive”. Experience tells us that although the surgical trauma to the nasal structures may be less, this technique requires a more extensive sphenoidotomy in order to assure full mobility of the endoscope and lack of collision with other instruments. In this respect it is actually more invasive, particularly when the turbinate is resected, a procedure which we find unnecessary in most cases.
There is debate about the use of intraoperative imaging and navigation. In training programs, these adjuncts may be valuable in the education of residents and fellows. There is also debate about whether all young neurosurgeons should follow this type of progressive approach or whether they should simply begin with the endoscopic methods that have proven to be so effective.
Edward Laws and John A Jane Jr
Rights and permissions
About this article
Cite this article
Duz, B., Harman, F., Secer, H.I. et al. Transsphenoidal approaches to the pituitary: a progression in experience in a single centre. Acta Neurochir (Wien) 150, 1133–1139 (2008). https://doi.org/10.1007/s00701-008-0135-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-008-0135-y