
Abstract
Purpose
To clarify the Japan criteria (JC), as proposed in 2019, in order to identify the most appropriate treatment methods for hepatocellular carcinoma (HCC) recurrence and assess the feasibility of pre-living donor liver transplantation (LDLT) downstaging within these criteria.
Methods
The subjects of this study were 169 LDLT patients with HCC recurrence. We performed univariate and multivariate analyses of the factors contributing to HCC recurrence after LDLT and clarified the post-transplant outcomes of pre-LDLT downstaging.
Results
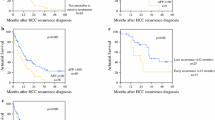
Univariate and multivariate analysis identified beyond the JC (p = 0.0018) and a neutrophil-to-lymphocyte ratio > 2.01 (p = 0.029) as independent risk factors. Patients who met the JC had significantly higher recurrence-free and overall survival rates after LDLT (p < 0.0001) than those who did not (p = 0.0002). The post-transplant outcomes of patients within the JC after downstaging were significantly better than those of patients beyond the JC (p = 0.034) and equivalent to those within the JC without downstaging.
Conclusion
Even for HCC recurrence, the JC could play an important role in deciding on the best treatment strategy, and downstaging within the JC had good post-transplant outcomes.



Similar content being viewed by others

References
Villanueva A. Hepatocellular carcinoma. N Engl J Med. 2019;380(15):1450–62.
Kudo M, Kawamura Y, Hasegawa K, Tateishi R, Kariyama K, Shiina S, et al. Management of hepatocellular carcinoma in Japan: JSH consensus statements and recommendations 2021 update. Liver Cancer. 2021;10(3):181–223.
Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693–9.
Shimamura T, Akamatsu N, Fujiyoshi M, Kawaguchi A, Morita S, Kawasaki S, et al. Expanded living-donor liver transplantation criteria for patients with hepatocellular carcinoma based on the Japanese nationwide survey: the 5-5-500 rule-a retrospective study. Transpl Int. 2019;32(4):356–68.
Tabrizian P, Holzner ML, Mehta N, Halazun K, Agopian VG, Yao F, et al. Ten-year outcomes of liver transplant and downstaging for hepatocellular carcinoma. JAMA Surg. 2022;157(9):779–88.
Tran NH, Muñoz S, Thompson S, Hallemeier CL, Bruix J. Hepatocellular carcinoma downstaging for liver transplantation in the era of systemic combined therapy with anti-VEGF/TKI and immunotherapy. Hepatology. 2022;76(4):1203–18.
Taketomi A, Sanefuji K, Soejima Y, Yoshizumi T, Uhciyama H, Ikegami T, et al. Impact of des-gamma-carboxy prothrombin and tumor size on the recurrence of hepatocellular carcinoma after living donor liver transplantation. Transplantation. 2009;87(4):531–7.
Toshima T, Yoshizumi T, Shimagaki T, Wang H, Kurihara T, Nagao Y, et al. Which is better to use “body weight” or “standard liver weight”, for predicting small-for-size graft syndrome after living donor liver transplantation? Ann Gastroenterol Surg. 2021;5(3):363–72.
Yonemura Y, Yoshizumi T, Inokuchi S, Kosai-Fujimoto Y, Harada N, Itoh S, et al. Predictor of outcome after living donor liver transplantation for patients with hepatocellular carcinoma beyond the Japan criteria. Ann Gastroenterol Surg. 2020;4(4):413–21.
Yoshiya S, Harada N, Tomiyama T, Takeishi K, Toshima T, Iguchi T, et al. The significant prognostic factors in prolonged intensive/high care unit stay after living donor liver transplantation. Transplant Proc. 2021;53(5):1630–8.
Yoshiya S, Shirabe K, Kimura K, Yoshizumi T, Ikegami T, Kayashima H, et al. The causes, risk factors, and outcomes of early relaparotomy after living-donor liver transplantation. Transplantation. 2012;94(9):947–52.
Xu L, Chen L, Zhang W. Neoadjuvant treatment strategies for hepatocellular carcinoma. World J Gastrointest Surg. 2021;13(12):1550–66.
Shimada M, Takenaka K, Taguchi K, Fujiwara Y, Gion T, Kajiyama K, et al. Prognostic factors after repeat hepatectomy for recurrent hepatocellular carcinoma. Ann Surg. 1998;227(1):80–5.
Yamashita Y, Shirabe K, Tsuijita E, Takeishi K, Ikegami T, Yoshizumi T, et al. Third or more repeat hepatectomy for recurrent hepatocellular carcinoma. Surgery. 2013;154(5):1038–45.
Yamashita Y, Yoshida Y, Kurihara T, Itoh S, Harimoto N, Ikegami T, et al. Surgical results for recurrent hepatocellular carcinoma after curative hepatectomy: Repeat hepatectomy versus salvage living donor liver transplantation. Liver Transpl. 2015;21(7):961–8.
Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–90.
Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–73.
Bruix J, Qin S, Merle P, Granito A, Huang YH, Bodoky G, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66.
Abou-Alfa GK, Meyer T, Cheng AL, El-Khoueiry AB, Rimassa L, Ryoo BY, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63.
Peng Z, Fan W, Zhu B, Wang G, Sun J, Xiao C, et al. Lenvatinib combined with transarterial chemoembolization as first-line treatment for advanced hepatocellular carcinoma: a phase III, randomized clinical trial (LAUNCH). J Clin Oncol. 2022;41(1):117–27.
Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–905.
Acuna SA, Zhang W, Yoon PD, Ivanics T, Zhu MP, Claasen M, et al. Right lobe versus left lobe living donor liver transplantation: a systematic review and meta-analysis of donor and recipient outcomes. Transplantation. 2022;106:2370.
Kulik L, Heimbach JK, Zaiem F, Almasri J, Prokop LJ, Wang Z, et al. Therapies for patients with hepatocellular carcinoma awaiting liver transplantation: a systematic review and meta-analysis. Hepatology. 2018;67(1):381–400.
Schwacha-Eipper B, Minciuna I, Banz V, Dufour JF. Immunotherapy as a downstaging therapy for liver transplantation. Hepatology. 2020;72(4):1488–90.
Nordness MF, Hamel S, Godfrey CM, Shi C, Johnson DB, Goff LW, et al. Fatal hepatic necrosis after nivolumab as a bridge to liver transplant for HCC: are checkpoint inhibitors safe for the pretransplant patient? Am J Transplant. 2020;20(3):879–83.
Qiao ZY, Zhang ZJ, Lv ZC, Tong H, Xi ZF, Wu HX, et al. Neoadjuvant programmed cell death 1 (PD-1) inhibitor treatment in patients with hepatocellular carcinoma before liver transplant: a cohort study and literature review. Front Immunol. 2021;12: 653437.
DiNorcia J, Florman SS, Haydel B, Tabrizian P, Ruiz RM, Klintmalm GB, et al. Pathologic response to pretransplant locoregional therapy is predictive of patient outcome after liver transplantation for hepatocellular carcinoma: analysis from the us multicenter hcc transplant consortium. Ann Surg. 2020;271(4):616–24.
Harding-Theobald E, Yao FYK, Mehta N. Neutrophil-to-lymphocyte ratio predicts high-risk explant features and waitlist survival but is not independently associated with recurrence or survival following liver transplantation for hepatocellular carcinoma. Liver Transpl. 2021;27(6):818–29.
Motomura T, Shirabe K, Mano Y, Muto J, Toshima T, Umemoto Y, et al. Neutrophil-lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment. J Hepatol. 2013;58(1):58–64.
Mano Y, Shirabe K, Yamashita Y, Harimoto N, Tsujita E, Takeishi K, et al. Preoperative neutrophil-to-lymphocyte ratio is a predictor of survival after hepatectomy for hepatocellular carcinoma: a retrospective analysis. Ann Surg. 2013;258(2):301–5.
Funding
This study was supported by the following three grants: the Program for Basic and Clinical Research on Hepatitis, from the Japan Agency for Medical Research and Development, AMED (Numbers 20fk0210035s0503, 20fk0310106h0204, and 19fm0208009h0003); JSPS KAKENHI Grant Numbers JP-18K08542; and Taiju Life Social Welfare Foundation 2020. The funding sources had no role in the collection, analysis, or interpretation of the data, or in the decision to submit the article for publication.
Author information
Authors and Affiliations
Contributions
SY participated in research design, data analysis, and writing of the manuscript. NH, TT, and TY contributed to the discussion and reviewed the manuscript. YN, HK, and SI participated in data analysis and interpretation. KT, YK, and T. Tomino participated in data collection.
Corresponding author
Ethics declarations
Conflict of interest
We have no conflicts of interest to declare.
Ethical approval
This retrospective study was approved by the ethics committee of Kyushu University (ID number: 2019–186).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yoshiya, S., Harada, N., Toshima, T. et al. Treatment strategy for hepatocellular carcinoma recurrence in the transplant era: Focusing on the Japan criteria. Surg Today 54, 64–72 (2024). https://doi.org/10.1007/s00595-023-02710-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-023-02710-z