
Abstract
Purpose
The precise role of downstaging or bridge therapy for cirrhotic patients with hepatocellular carcinoma (HCC) beyond or within the Milan criteria (MC) before living donor liver transplantation (LDLT) remains undefined.
Methods
We conducted a single-center, retrospective cohort study of 40 cirrhotic patients with HCC who underwent LDLT from 2000 to 2018. Dynamic computed tomography images at the initial presentation and immediately before LDLT as well as the final histopathological findings were reviewed to determine whether they met or exceeded MC.
Results
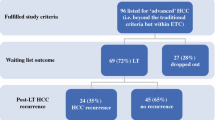
Overall, 29 patients underwent various pre-transplant HCC treatments, including ablation and embolization (bridge therapy, n = 20; downstaging, n = 9). Of the 9 patients who were initially beyond the MC, 4 (44.4%) were successfully downstaged to within the MC. Five patients beyond the MC immediately before LDLT demonstrated a significantly worse 5-year overall survival rate than patients within the MC (16.7% vs. 82.2%, P = 0.004), regardless of the radiological HCC stage at presentation or the final pathological tumor status. All 3 recurrent patients had HCC beyond the MC immediately before transplant and died of their disease at 13, 24, and 50 months after transplantation.
Conclusions
Successful downstaging for HCC cases beyond the MC provides similar outcomes to those within the MC at presentation, regardless of the histopathological findings.



Similar content being viewed by others


References
Huang J, Yan L, Cheng Z, Wu H, Du L, Wang J, et al. A randomized trial comparing radiofrequency ablation and surgical resection for HCC conforming to the Milan criteria. Ann Surg. 2010;252:903–12.
Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020–2.
Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–9.
Shetty K, Timmins K, Brensinger C, Furth EE, Rattan S, Sun W, et al. Liver transplantation for hepatocellular carcinoma validation of present selection criteria in predicting outcome. Liver Transpl. 2004;10:911–8.
Llovet JM. Updated treatment approach to hepatocellular carcinoma. J Gastroenterol. 2005;40:225–35.
Kim PT, Onaca N, Chinnakotla S, Davis GL, Jennings LW, Mckenna GJ, et al. Tumor biology and pre-transplant locoregional treatments determine outcomes in patients with T3 hepatocellular carcinoma undergoing liver transplantation. Clin Transplant. 2013;27:311–8.
Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33:1394–403.
Yao FY, Ferrell L, Bass NM, Bacchetti P, Ascher NL, Roberts JP. Liver transplantation for hepatocellular carcinoma: comparison of the proposed UCSF criteria with the Milan criteria and the Pittsburgh modified TNM criteria. Liver Transpl. 2002;8:765–74.
Kwon CH, Kim DJ, Han YS, Park JB, Choi GS, Kim SJ, et al. HCC in living donor liver transplantation: can we expand the Milan criteria? Dig Dis. 2007;25:313–9.
Xu X, Ke QH, Shao ZX, Wu J, Chen J, Zhou L, et al. The value of serum alpha-fetoprotein in predicting tumor recurrence after liver transplantation for hepatocellular carcinoma. Dig Dis Sci. 2009;54:385–8.
Ito T, Takada Y, Ueda M, Haga H, Maetani Y, Oike F, et al. Expansion of selection criteria for patients with hepatocellular carcinoma in living donor liver transplantation. Liver Transpl. 2007;13:1637–44.
Chan SC, Fan ST. Selection of patients of hepatocellular carcinoma beyond the Milan criteria for liver transplantation. Hepatobiliary Surg Nutr. 2013;2:84–8.
Menon KV, Hakeem AR, Heaton ND. Review article: liver transplantation for hepatocellular carcinoma: a critical appraisal of the current worldwide listing criteria. Aliment Pharmacol Ther. 2014;40:893–902.
Hammad A, Kaido T, Ogawa K, Fujimoto Y, Uemura T, Mori A, et al. Liver transplantation for advanced hepatocellular carcinoma in patients with Child-Pugh A and B. Surg Today. 2016;46:248–54.
Mazzaferro V, Llovet JM, Miceli R, Bhoori S, Schiavo M, Mariani L, et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 2009;10:35–433.
Shimamura T, Akamatsu N, Fujiyoshi M, Kawaguchi A, Morita S, Kawasaki S, et al. Expanded living-donor liver transplantation criteria for patients with hepatocellular carcinoma based on the Japanese nationwide survey: the 5-5-500 rule: a retrospective study. Transpl Int. 2019;32:356–68.
El-Gazzaz G, Sourianarayanane A, Menon KVN, Sanabria J, Hashimoto K, Quintini C, et al. Radiologic-histological correlation of hepatocellular carcinoma treated via pre-liver transplant locoregional therapies. Hepatobiliary Pancreat Dis Int. 2013;12:34–41.
Ogawa K, Kaido T, Okajima H, Fujimoto Y, Yoshizawa A, Yagi S, et al. Impact of pretreatments on outcomes after living donor liver transplantation for hepatocellular carcinoma. J Hepatobiliary Pancreat Sci. 2019;26:73–81.
Lei J, Wang W, Yan L. Downstaging advanced hepatocellular carcinoma to the Milan criteria may provide a comparable outcome to conventional Milan criteria. J Gastrointest Surg. 2013;17:1440–6.
Yao FY, Xiao L, Bass NM, Kerlan R, Ascher NL, Roberts JP. Liver transplantation for hepatocellular carcinoma: validation of the UCSF-expanded criteria based on preoperative imaging. Am J Transplant. 2007;7:2587–96.
Sourianarayanane A, El-Gazzaz G, Sanabria JR, Menon KV, Quintini C, Hashimoto K, et al. Loco-regional therapy in patients with Milan Criteria-compliant hepatocellular carcinoma and short waitlist time to transplant: an outcome analysis. HPB (Oxford). 2012;14:325–32.
Chan KM, Yu MC, Chou HS, Wu TJ, Lee CF, Lee WC. Significance of tumor necrosis for outcome of patients with hepatocellular carcinoma receiving locoregional therapy prior to liver transplantation. Ann Surg Oncol. 2011;18:2638–46.
Lei J, Yan L, Wang W. Comparison of the outcomes of patients who underwent deceased-donor or living-donor liver transplantation after successful downstaging therapy. Eur J Gastroenterol Hepatol. 2013;25:1340–6.
Takada Y, Ito T, Ueda M, Sakamoto S, Haga H, Maetani Y, et al. Living donor liver transplantation for patients with HCC exceeding the Milan criteria: a proposal of expanded criteria. Dig Dis. 2007;25:299–302.
Yao FY, Breitenstein S, Broelsch CE, Dufour JF, Sherman M. Does a patient qualify for liver transplantation after the down-staging of hepatocellular carcinoma? Liver Transpl. 2011;17(Suppl 2):S109–S116116.
Yao FY, Kinkhabwala M, Laberge JM, Bass NM, Brown R Jr, Kerlan R, et al. The impact of pre-operative loco-regional therapy on outcome after liver transplantation for hepatocellular carcinoma. Am J Transplant. 2005;5:795–804.
Cillo U, Vitale A, Grigoletto F, Gringeri E, D'amico F, Valmasoni M, et al. Intention-to-treat analysis of liver transplantation in selected, aggressively treated HCC patients exceeding the Milan criteria. Am J Transplant. 2007;7:972–81.
Cescon M, Cucchetti A, Ravaioli M, Pinna AD. Hepatocellular carcinoma locoregional therapies for patients in the waiting list. Impact on transplantability and recurrence rate. J Hepatol. 2013;58:609–18.
Yao FY, Jr. KerlanHirose RKR, Davern TJ, Bass NM, Feng S, et al. Excellent outcome following down-staging of hepatocellular carcinoma prior to liver transplantation: an intention-to-treat analysis. Hepatology. 2008;48:819–27.
Ravaioli M, Grazi GL, Piscaglia F, Trevisani F, Cescon M, Ercolani G, et al. Liver transplantation for hepatocellular carcinoma: results of down-staging in patients initially outside the Milan selection criteria. Am J Transplant. 2008;8:2547–57.
Sumie S, Kuromatsu R, Okuda K, Ando E, Takata A, Fukushima N, et al. Microvascular invasion in patients with hepatocellular carcinoma and its predictable clinicopathological factors. Ann Surg Oncol. 2008;15:1375–82.
Pawlik TM, Delman KA, Vauthey JN, Nagorney DM, Ng IO, Ikai I, et al. Tumor size predicts vascular invasion and histologic grade: Implications for selection of surgical treatment for hepatocellular carcinoma. Liver Transpl. 2005;11:1086–92.
Riaz A, Kulik L, Lewandowski RJ, Ryu RK, Giakoumis Spear G, Mulcahy MF, et al. Radiologic-pathologic correlation of hepatocellular carcinoma treated with internal radiation using yttrium-90 microspheres. Hepatology. 2009;49:1185–93.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
595_2020_2095_MOESM1_ESM.pdf
Supplementary file1 (PDF 187 kb) Supplementary Fig. S1 (Online Resource 1). The overall survival of patients with and without locoregional therapy before transplantation. The 5-year survival rates of patients with (n = 29) and without (n = 11) locoregional therapy were 68.0% and 72.7%, respectively. This difference was not statistically significant (P = 0.872).
595_2020_2095_MOESM2_ESM.pdf
Supplementary file2 (PDF 188 kb) Supplementary Fig. S2 (Online Resource 2). The overall survival of patients pathologically within and beyond Milan criteria. The 5-year survival rates of patients within (n = 18) and beyond (n = 22) Milan criteria were 83.3% and 65.7%, respectively. This difference was not statistically significant (P = 0.325).
595_2020_2095_MOESM3_ESM.pdf
Supplementary file3 (PDF 188 kb) Supplementary Fig. S3 (Online Resource 3). The overall survival of patients with and without vascular invasion. The survival rate of patients with vascular invasion (n = 17) was significantly lower than that of patients without invasion (n = 23; P = 0.020).
Rights and permissions
About this article

Cite this article
Inomata, K., Yagi, H., Hibi, T. et al. Long-term outcomes of living donor liver transplantation after locoregional treatment for hepatocellular carcinoma: an experience from a single institute. Surg Today 51, 350–357 (2021). https://doi.org/10.1007/s00595-020-02095-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-020-02095-3