
Abstract
Purpose
Familial adenomatous polyposis (FAP)-associated desmoid tumor (DT) is sometimes life threatening. However, the optimal treatment for DTs has not been established. The aim of this study was to analyze the outcomes of surgical and pharmacological treatments for DT in Japanese FAP patients.
Methods
We retrospectively reviewed the data of 303 patients who underwent colectomy for FAP between 2000 and 2012. We analyzed 41 patients with DTs in which the location was apparent. The selection of treatment for intra-abdominal DTs was also evaluated according to Church’s classification.
Results
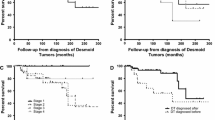
Surgery was frequently used to treat extra-abdominal DTs. Multimodal treatments, including surgery, and the administration of non-steroidal anti-inflammatory drugs, hormonal therapy, and chemotherapy were widely used for intra-abdominal DTs. The most effective pharmacological treatment was cytotoxic chemotherapy, which was associated with a response rate of 45.5% and a disease control rate of 72.7%. After a median follow-up period of 53.0 months, the 5-year DT-specific survival rate in patients with stage IV disease was 71.4%; in contrast, the rate in patients with other stages was 100%. Four-stage IV patients died of DT due to uncontrollable rapid progression. No cytotoxic chemotherapy was administered; however, incomplete resection was performed in three cases.
Conclusion
Our findings will provide clues that may help physicians in selecting the optimal strategy for this rare disease.


Similar content being viewed by others


References
Hata K, Yamamoto Y, Kiyomatsu T, Tanaka T, Kazama S, Nozawa H, et al. Hereditary gastrointestinal cancer. Surg Today. 2016;46:1115–22.
Sturt NJ, Clark SK. Current ideas in desmoid tumours. Fam Cancer. 2006;5:275–85.
Sinha A, Tekkis PP, Gibbons DC, Phillips RK, Clark SK. Risk factors predicting desmoid occurrence in patients with familial adenomatous polyposis: a meta-analysis. Colorectal Dis. 2011;13:1222–9.
de Campos FG, Perez RO, Imperiale AR, Seid VE, Nahas SC, Cecconello I. Evaluating causes of death in familial adenomatous polyposis. J Gastrointest Surg. 2010;14:1943–9.
Clark SK, Neale KF, Landgrebe JC, Phillips RK. Desmoid tumours complicating familial adenomatous polyposis. Br J Surg. 1999;86:1185–9.
Latchford AR, Sturt NJ, Neale K, Rogers PA, Phillips RK. A 10-year review of surgery for desmoid disease associated with familial adenomatous polyposis. Br J Surg. 2006;93:1258–64.
Soravia C, Berk T, McLeod RS, Cohen Z. Desmoid disease in patients with familial adenomatous polyposis. Dis Colon Rectum. 2000;43:363–9.
Berk T, Cohen Z, McLeod RS, Stern HS. Management of mesenteric desmoid tumours in familial adenomatous polyposis. Can J Surg. 1992;35:393–5.
Schnitzler M, Cohen Z, Blackstein M, Berk T, Gallinger S, Madlensky L, et al. Chemotherapy for desmoid tumors in association with familial adenomatous polyposis. Dis Colon Rectum. 1997;40:798–801.
Gega M, Yanagi H, Yoshikawa R, Noda M, Ikeuchi H, Tsukamoto K, et al. Successful chemotherapeutic modality of doxorubicin plus dacarbazine for the treatment of desmoid tumors in association with familial adenomatous polyposis. J Clin Oncol. 2006;24:102–5.
Desurmont T, Lefèvre JH, Shields C, Colas C, Tiret E, Parc Y. Desmoid tumour in familial adenomatous polyposis patients: responses to treatments. Fam Cancer. 2015;14:31–9.
Church J, Lynch C, Neary P, LaGuardia L, Elayi E. A desmoid tumor-staging system separates patients with intra-abdominal, familial adenomatous polyposis-associated desmoid disease by behavior and prognosis. Dis Colon Rectum. 2008;51:897–901.
Nieuwenhuis MH, Lefevre JH, Bülow S, Järvinen H, Bertario L, Kernéis S, et al. Family history, surgery, and APC mutation are risk factors for desmoid tumors in familial adenomatous polyposis: an international cohort study. Dis Colon Rectum. 2011;54:1229–34.
Lynch HT, Fitzgibbons R Jr. Surgery, desmoid tumors, and familial adenomatous polyposis: case report and literature review. Am J Gastroenterol. 1996;91:2598–601.
Smith AJ, Lewis JJ, Merchant NB, Leung DH, Woodruff JM, Brennan MF. Surgical management of intra-abdominal desmoid tumours. Br J Surg. 2000;87:608–13.
Colombo C, Foo WC, Whiting D, Young ED, Lusby K, Pollock RE, et al. FAP-related desmoid tumors: a series of 44 patients evaluated in a cancer referral center. Histol Histopathol. 2012;27:641–9.
Vasen HF, Möslein G, Alonso A, Aretz S, Bernstein I, Bertario L, et al. Guidelines for the clinical management of familial adenomatous polyposis (FAP). Gut. 2008;57:704–13.
Nieuwenhuis MH, Mathus-Vliegen EM, Baeten CG, Nagengast FM, van der Bijl J, van Dalsen AD, et al. Evaluation of management of desmoid tumours associated with familial adenomatous polyposis in Dutch patients. Br J Cancer. 2011;104:37–42.
Quast DR, Schneider R, Burdzik E, Hoppe S, Möslein G. Long-term outcome of sporadic and FAP-associated desmoid tumors treated with high-dose selective estrogen receptor modulators and sulindac: a single-center long-term observational study in 134 patients. Fam Cancer. 2016;15:31–40.
Tsukada K, Church JM, Jagelman DG, Fazio VW, Lavery IC. Systemic cytotoxic chemotherapy and radiation therapy for desmoid in familial adenomatous polyposis. Dis Colon Rectum. 1991;34:1090–2.
Patel SR, Benjamin RS. Desmoid tumors respond to chemotherapy: defying the dogma in oncology. J Clin Oncol. 2006;24:11–2.
Lynch HT, Fitzgibbons R Jr, Chong S, Cavalieri J, Lynch J, Wallace F, et al. Use of doxorubicin and dacarbazine for the management of unresectable intra-abdominal desmoid tumors in Gardner’s syndrome. Dis Colon Rectum. 1994;37:260–7.
Hamilton L, Blackstein M, Berk T, McLeod RS, Gallinger S, Madlensky L, et al. Chemotherapy for desmoid tumours in association with familial adenomatous polyposis: a report of three cases. Can J Surg. 1996;39:247–52.
Poritz LS, Blackstein M, Berk T, Gallinger S, McLeod RS, Cohen Z. Extended follow-up of patients treated with cytotoxic chemotherapy for intra-abdominal desmoid tumors. Dis Colon Rectum. 2001;44:1268–73.
Yamamoto H, Oshiro R, Nishimura J, Uemura M, Haraguchi N, Hata T, et al. Low-dose dacarbazine-doxorubicin therapy against intra-abdominal desmoid tumors. Oncol Rep. 2013;29:1751–5.
Weiss AJ, Lackman RD. Low-dose chemotherapy of desmoid tumors. Cancer. 1989;64:1192–4.
Skapek SX, Hawk BJ, Hoffer FA, Dahl GV, Granowetter L, Gebhardt MC et al. Combination chemotherapy using vinblastine and methotrexate for the treatment of progressive desmoid tumor in children. J Clin Oncol. 1998;16:3021–7.
Reich S, Overberg-Schmidt US, Bührer C, Henze G. Low-dose chemotherapy with vinblastine and methotrexate in childhood desmoid tumors. J Clin Oncol. 1999;17:1086.
Azzarelli A, Gronchi A, Bertulli R, Tesoro JD, Baratti D, Pennacchioli E, et al. Low-dose chemotherapy with methotrexate and vinblastine for patients with advanced aggressive fibromatosis. Cancer. 2001;92:1259–64.
Weiss AJ, Horowitz S, Lackman RD. Therapy of desmoid tumors and fibromatosis using vinorelbine. Am J Clin Oncol. 1999;22:193–5.
Ezumi K, Yamamoto H, Takemasa I, Nomura M, Ikeda M, Sekimoto M, et al. Dacarbazine-Doxorubicin therapy ameliorated an extremely aggressive mesenteric desmoid tumor associated with familial adenomatous polyposis: report of a case. Jpn J Clin Oncol. 2008;38:222–6.
Slowik V, Attard T, Dai H, Shah R, Septer S. Desmoid tumors complicating Familial Adenomatous Polyposis: a meta-analysis mutation spectrum of affected individuals. BMC Gastroenterol. 2015;15:84.
Acknowledgements
The authors would like to acknowledge all of the patients and their families. In addition to the investigators in the author list, we acknowledge the following investigators who participated in this study: Koji Komori, Department of Gastroenterological Surgery Aichi Cancer Center Hospital, Aichi; Kenjiro Kotake, Department of Surgery, Tochigi Cancer Center, Tochigi; Takeshi Nagasaka, Department of Gastroenterological Surgery, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama; Hirotoshi Hasegawa, Department of Surgery, Keio University School of Medicine, Tokyo; Motoi Koyama, Department of Gastroenterological Surgery, Hirosaki University Graduate School of Medicine, Aomori; Yoshito Akagi, Department of Surgery, Kurume University School of Medicine, Kurume, Fukuoka; Toshimasa Yatsuoka, Department of Gastroenterological Surgery, Saitama Cancer Center, Saitama; Masataka Ikeda, Department of Surgery, National Hospital Organization, Osaka National Hospital, Osaka; Kensuke Kumamoto, Department of Organ Regulatory Surgery, Fukushima Medical University School of Medicine, Fukushima; Kiyotaka Kurachi, Department of Surgery 2, Hamamatsu University School of Medicine, Shizuoka;Toshiaki Watanabe, Department of Surgical Oncology, Graduate School of Medicine, The University of Tokyo, Tokyo; Kohji Tanakaya, Department of Surgery, Iwakuni Clinical Center, Yamaguchi; Kazuhiko Yoshimatsu, Department of Surgery, Tokyo Women’s Medical University Medical Center East, Tokyo.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The present study was supported in part by a grant-in-aid for Cancer Research from the Ministry of Health, Labor and Welfare, and by the Japanese Society for Cancer of the Colon and Rectum.
Conflict of interest
The authors declare no conflicts of interest in association with the present study.
Rights and permissions
About this article

Cite this article
Inoue, Y., Ishida, H., Ueno, H. et al. The treatment of desmoid tumors associated with familial adenomatous polyposis: the results of a Japanese multicenter observational study. Surg Today 47, 1259–1267 (2017). https://doi.org/10.1007/s00595-017-1500-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-017-1500-3