
Abstract
Purpose
The Estimation of Physiologic Ability and Surgical Stress (E-PASS) scoring system, which quantifies a patient’s reserve and surgical stress, is used to predict morbidity and mortality in patients before elective gastrointestinal surgery. We conducted this study to clarify whether the E-PASS scoring system is useful for assessing the risks of emergency abdominal surgery.
Methods
The subjects of this retrospective study were 51 patients who underwent emergency gastrointestinal surgery at a public general hospital. The main outcomes were the E-PASS scores and the postoperative course, defined by mortality and morbidity.
Results
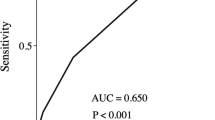
Postoperative complications developed in 15 of the 51 patients (29.4%). The E-PASS score was significantly higher in the patients with postoperative complications than in those without (0.61 ± 0.31 vs 0.20 ± 0.35, respectively; n = 36). The morbidity rates were significantly lower in the patients with a value less than 0.5 than in those with a value more than 0.5 (17.1% and 56.3%, respectively; P < 0.01). There were 7 operative deaths among the 16 patients with a high score, versus none among the 9 patients with a low score (P < 0.01). Three patients underwent laparoscopic-assisted bowel resection with a good postoperative course, with scores of less than 0.5.
Conclusions
The E-PASS scoring system is useful for surgical decision making and evaluating whether patients will tolerate emergency gastrointestinal surgery. Minimally invasive therapy would assist in lowering the risk of complications.
Similar content being viewed by others


References
Copeland GP, Jones D, Walters M. POSSUM: A scoring system for surgical audit. Br J Surg 1991;78:356–60.
Haga Y, Wada Y, Takeuchi H, Kimura O, Furuya T, Sameshima H, et al. Estimation of physiologic ability and surgical stress (E-PASS) for a surgical audit in elective digestive surgery. Surgery 2004;135: 586–594.
Hashimoto D, Takamori H, Sakamoto Y, Tanaka H, Hirota M, Baba H. Can the physiologic ability and surgical stress (E-PASS) scoring system predict operative morbidity after distal pancreatectomy? Surg Today 2010;40:632–637.
Common Toxicity Criteria, Version 2.0. April 30, 1999.
Haga Y, Ikei S, Ogawa M. Estimation of Physiologic Ability and Surgical Stress (E-PASS) as a new prediction scoring system for postoperative morbidity and mortality following elective gastrointestinal surgery. Surg Today 1999;29:219–225.
Pappachan JV, Millar B, Bennett ED, Smith GB. Comparison of outcome from intensive care admission after adjustment for case mix by the APACHE II prognostic system. Chest 1999;115: 802–810.
Midwinter MJ, Tytherleigh M, Ashley S. Estimation of mortality and morbidity risk in vascular surgery using POSSUM and the Portsmouth predictor equation. Br J Surg 1999;86:471–474.
Kumar P, Rodrigues GS. Comparison of POSSUM and P-POSSUM for risk-adjusted audit of patients undergoing emergency laparotomy. Ulus Trauma Acil Cerrahi Derg 2009;15:19–22.
Gój K, Knapik P, Kucewicz-Czech E, Luboń D. The Therapeutic Intervention Scoring System (TISS-28) for assessment of cardiac surgical postoperative intensive care. Anestezjol Intens Ter 2009; 41:34–37.
Dossett LA, Redhage LA, Sawyer RG, May AK. Revisiting the validity of APACHE II in the trauma ICU: improved risk stratification in critically injured adults. Injury 2009;40:993–998.
Pappachan JV, Millar B, Bennett ED, Smith GB. Comparison of outcome from intensive care admission after adjustment for case mix by the APACHE II prognostic system. Chest 1999;115: 802–810.
Midwinter MJ, Tytherleigh M, Ashley S. Estimation of mortality and morbidity risk in vascular surgery using POSSUM and the Portsmouth predictor equation. Br J Surg 1999;86:471–474.
Kanus WA, Draper EA, Wagner DP, Zimmerman JE. Apache II: a severity of disease classification system. Crit Care Med 1985;13:818–829.
Haga Y, Yagi Y, Ogawa M. Less-invasive surgery for gastric cancer prolongs survival in patients over 80 years of age. Surg Today 1999;29:842–848.
Author information
Authors and Affiliations
Additional information
This paper was presented at the 62nd Annual Meeting of the Japanese Society of Gastroenterological Surgery in Tokyo, Japan, on July 19, 2007.
Rights and permissions
About this article
Cite this article
Koushi, K., Korenaga, D., Kawanaka, H. et al. Using the E-PASS scoring system to estimate the risk of emergency abdominal surgery in patients with acute gastrointestinal disease. Surg Today 41, 1481–1485 (2011). https://doi.org/10.1007/s00595-010-4538-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-010-4538-z