
Abstract
Background
A long global thoracolumbar kyphosis is common in ankylosing spondylitis. Surgical correction of fixed sagittal malalignment by pedicle subtraction osteotomy (PSO) might improve disability and quality of life (QoL). Two-level osteotomies represent major procedures with a risk of hemorrhage. Combined open and minimal invasive surgery has not been described and might be considered.
Case presentation
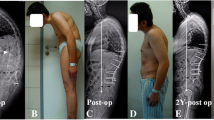
A 30-year-old female with ankylosing spondylitis was treated by golimumab and teriparatide. The treatment was stopped during pregnancy which led to vertebral compression fractures and kyphosis of 50° between T11 and L3. A PSO was planned at the kyphotic apex L2. The second PSO was planned at L4 according to the pelvic incidence of 56°, matching with a spinopelvic alignment Roussouly type 3. A derived full balance integrated method was used to calculate the amount of correction. During the first stage surgery, an open approach was performed from L1 to pelvis and combined with percutaneous cement-augmented instrumentation in already fused segments T5–T12, thus reducing perioperative morbidity. A stepwise approach including L2 PSO closure with temporary rods and L4 PSO with final instrumentation was used. Blood loss was estimated around 1100 ml. The patient was able to walk on the second day after surgery. A secondary anterior fusion with LLI cages from L2 to L5 and an ALIF at L5–S1 were performed because of high non-ossified intervertebral disks to reduce the risk for nonunion and rod fractures. At 2-year follow-up, the patient’s QoL had significantly improved and full spine radiographs showed stable normalized sagittal parameters.
Conclusion
The combined open and percutaneous approach was feasible and might be considered as an alternative option to conventional open surgery when planning major deformity correction in ankylosing spondylitis.










Similar content being viewed by others


Abbreviations
- PSO:
-
Pedicle subtraction osteotomy
- QoL:
-
Quality of life
- LLI:
-
Lumbar lateral interbody
- ALIF:
-
Anterior lumbar interbody fusion
- TNF:
-
Tumor necrosis factor
- VAS:
-
Visual analogue scale
- SVA:
-
Sagittal vertical axis
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- FBI:
-
Full balance integrated
- PMMA:
-
Polymethyl-methacrylate
- CBVA:
-
Chin–brow vertical angle
- ODI:
-
Oswestry Disability Index
- mSASSS:
-
Modified stokes ankylosing spondylitis spinal score
- SRS:
-
Scoliosis Research Society
- PJK:
-
Proximal junctional kyphosis
References
Koller H, Koller J, Mayer M, Hempfing A, Hitzl W (2018) Osteotomies in ankylosing spondylitis: where, how many, and how much? Eur Spine J 27(Supplement 1):70–100
Kiaer T, Gehrchen M (2010) Transpedicular closed wedge osteotomy in ankylosing spondylitis: results of surgical treatment and prospective outcome analysis. Eur Spine J 19(1):57–64
Zheng G, Song K, Yao Z, Zhang Y, Tang X, Wang Z, Zhang X, Mao K, Cui G, Wang Y (2016) How to calculate the exact angle for two-level osteotomy in ankylosing spondylitis? Spine 41(17):E1046–E1052
Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ (2002) Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine 27(6):612–618
Hua WB, Zhang YK, Gao Y, Liu XZ, Yang SH, Wu XH, Wang J, Yang C (2017) Analysis of sagittal parameters in patients undergoing one- or two-level closing wedge osteotomy for correcting thoracolumbar kyphosis secondary to ankylosing spondylitis. Spine 42(14):E848–E854
Zheng GQ, Song K, Zhang YG, Wang Y, Huang P, Zhang XS, Wang Z, Mao KY, Cui G (2014) Two-level spinal osteotomy for severe thoracolumbar kyphosis in ankylosing spondylitis: experience with 48 patients. Spine 39(13):1055–1058
Xu H, Zhang Y, Zhao Y, Wang Z, Zhang X, Wang Y (2015) Radiologic and clinical outcomes comparison between single- and two-level pedicle subtraction osteotomies in correcting ankylosing spondylitis kyphosis. Spine J 15:290–297
Liu C, Yu W, Zheng G, Guo Y, Song K, Tang X, Wang Z, Wang Y, Zhang Y (2017) The safe correction angle of osteotomy at T12 and L1 for ankylosing spondylitis kyphosis: patients with 2-level osteotomy. Clin Spine Surg 30(7):E942–E947
Zhao Y, Wang Y, Wang Z, Zhang X, Mao K, Zhang Y (2017) Effect and strategy of 1-stage interrupted 2-level transpedicular wedge osteotomy for correcting severe kyphotic deformities in ankylosing spondylitis. Clin Spine Surg 30(4):E454–E459
Zhao SZ, Qian BP, Qiu Y, Qiao M, Liu ZJ, Huang JC (2019) The relationship between global spinal alignment and pelvic orientation from standing to sitting following pedicle subtraction osteotomy in ankylosing spondylitis patients with thoracolumbar kyphosis. Arch Orthop Trauma Surg 139(6):761–768
Van Royen BJ, De Gast A, Smit TH (2000) Deformity planning for sagittal plane corrective osteotomies of the spine in ankylosing spondylitis. Eur Spine J 9:492–498
Liu C, Zheng G, Guo Y, Song K, Tang X, Zhang X, Wang Z, Wang Y (2018) Two-level osteotomy for correcting severe ankylosing spondylitis kyphosis: radiologic outcomes of different osteotomy position-selection strategy for different type of patients. Spine Deform 6(3):273–281
Qiao M, Qian BP, Zhao SZ, Qiu Y, Wang B, Jiang J (2018) Clinical and radiographic results after posterior wedge osteotomy for thoracolumbar kyphosis secondary to ankylosing spondylitis: comparison of long and short segment. World Neurosurg 117:e475–e482
Zhang H, Zhang X, Hu F, Hu W, Wang Y, Hao Y (2018) Ankylosing spondylitis kyphosis surgical correction postoperative evaluation via SRS-22 domain investigation. J Orthop Surg Res 13(1):5
Zhao Y, Xu H, Zhang Y, Wang Z, Zhang X, Wang Y (2015) Comparison of two surgeries in treatment of severe kyphotic deformity caused by ankylosing spondylitis: transpedicular bivertebrae wedge osteotomy versus one-stage interrupted two-level transpedicular wedge osteotomy. Clin Neurol Neurosurg 139:252–257
Roussouly P, Gollogly S, Berthonnaud E, Dimnet J (2005) Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine 30(3):346–353
Le Huec JC, Leijssen P, Duarte M, Aunoble S (2011) Thoracolumbar imbalance analysis for osteotomy planification using a new method: FBI technique. Eur Spine J 20(Suppl 5):S669–S680
Wang T, Zhao Y, Liang Y, Zhang H, Wang Z, Wang Y (2018) Risk factor analysis of proximal junctional kyphosis after posterior osteotomy in patients with ankylosing spondylitis. J Neurosurg Spine 29(1):75–80
Mao SH, Feng ZX, Qian BP, Qiu Y (2018) The clinical relevance of the presence of bridging syndesmophytes on kyphosis correction and maintenance following pedicle subtraction osteotomy for thoracolumbar kyphotic deformity in ankylosing spondylitis: a comparative cohort study. BMC Muscoloskelet Disord 19(1):97
Zhao SZ, Qian BP, Qiao M, Jiang J, Qiu Y (2019) Does solid fusion eliminate rod fracture after pedicle subtraction osteotomy in ankylosing spondylitis-related thoracolumbar kyphosis? Spine J 19(1):79–86
Author information
Authors and Affiliations
Contributions
YPC contributed to manuscript writing, treatment and clinical follow-up of patient, YN contributed to manuscript review, treatment and clinical follow-up of patient, AC contributed to manuscript review, treatment and clinical follow-up of patient, JPS contributed to manuscript review and supervision.
Corresponding author
Ethics declarations
Conflict of interest
None of the authors have any potential conflict of interest directly related to this article.
Informed consent
The patient was informed that data from the case would to be submitted for publication and gave her consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Charles, Y.P., Ntilikina, Y., Collinet, A. et al. Combined percutaneous and open instrumentation for thoracolumbar kyphosis correction by two-level pedicle subtraction osteotomy in ankylosing spondylitis. Eur J Orthop Surg Traumatol 30, 939–947 (2020). https://doi.org/10.1007/s00590-020-02631-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-020-02631-4