
Abstract
Introduction
Quadriceps tendon avulsions are typically treated by reattaching the tendon through bone tunnels, with or without tendon or hardware augmentation. The operated knee joint can be moved right away; however, tendon grafting or tension banding will be required to protect the repair, and the hardware must be removed later on. The goal of this study was to evaluate the clinical and functional outcomes when suture anchors are used to reattached torn quadriceps tendon, and also to assess tendon healing using MRI.
Materials and methods
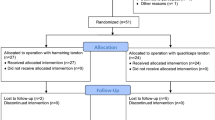
Thirteen consecutive patients with avulsed quadriceps tendons were operated and then followed prospectively. The surgical technique consisted of tendon reattachment using at least three anchors, in addition to intratendinous weaving of the sutures. Weight bearing was allowed while using a splint. Rehabilitation was initiated immediately after surgery according to a set protocol.
Results
Eleven patients were followed for a mean of 14.7 months. Two retears occurred in patients who did not wear the splint. Eighty-two per cent of patients were satisfied or very satisfied with the outcome. The mean knee flexion was 124.5°. All patients were able to return to their pre-injury activity levels. The mean time for clinical and functional recovery was 3 months. MRI performed 6 months after the surgical repair revealed good tendon healing.
Discussion
This was the first prospective study performed on quadriceps avulsion patients undergoing suture anchor repair. Prior clinical case reports have shown that this method leads to predictable clinical and functional results. Our results were comparable to those in published cases.
Conclusion
The procedure is simpler when only suture anchors are used. Tendon healing was observed on MRI in all cases. This simple, reproducible technique is free of the drawbacks associated with the typical repair augmentation.








Similar content being viewed by others


References
Clayton RAE, Court-Brown CM (2008) The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury 39(12):1338–1344
Konrath GA, Chen D, Lock T (1998) Outcomes following repair of quadriceps tendon ruptures. J Orthop Trauma 12(4):273–279
Levy M, Goldstein J, Rosner M (1987) A method of repair for quadriceps tendon or patellar ligament ruptures without cast immobilization: preliminary report. Clin Orthop Relat Res 218:297–301
De Baere T, Geulette B, Manche E (2002) Functional results after surgical repair of quadriceps tendon rupture. Acta Orthop Belg 68(2):146–149
Langenhan R, Baumann M, Ricart P (2012) Postoperative functional rehabilitation after repair of quadriceps tendon ruptures: a comparison of two different protocols. Knee Surg Sports Traumatol Arthrosc 20:2275–2278
Maniscalco P, Bertone C, Bonci E (1998) Titanium anchors for the repair of distal Achilles tendon ruptures: preliminary report of a new surgical technique. J Foot Ankle Surg 37(2):96–100
Maniscalco P, Bertone C, Rivera F (2000) A new method of repair for quadriceps tendon ruptures: a case report. Panminerva Med 42(3):223–225
Richards DP, Barber A (2002) Repair of quadriceps tendon ruptures using suture anchors. Arthroscopy 18(5):556–559
Kerin C, Hopgood P, Banks AJ (2006) Delayed repair of quadriceps using the Mitek anchor system: a case report and review of the literature. Knee 13:161–163
Bushnell BD, Whitener GB, Rubright JH (2007) The use of suture anchors to repair the ruptured quadriceps tendon. J Orthop Trauma 21(6):407–413
Howe TE, Dawson LJ, Syme G, Duncan L, Reid J (2012) Evaluation of outcome measures for use in clinical practice for adults with musculoskeletal conditions of the knee: a systematic review. Man Ther 17(2):100–118
Tegner Y, Lysholm J (1985) Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 198:43–49
Noyes FR, Barber SD, Mooar LA (1989) A rationale for assessing sports activity levels and limitations in knee disorders. Clin Orthop Relat Res 246:238–249
Cincinnati Score—Orthopaedic Scores [Internet]. [cited 2014 Aug 17]. http://www.orthopaedicscore.com/scorepages/cincinnati.html
Bentley G, Biant LC, Carrington RW, Akmal M, Goldberg A, Williams AM, Skinner JA, Pringle J (2003) A prospective, randomised comparison of autologous chondrocyte implantation versus mosaicplasty for osteochondral defects in the knee. J Bone Jt Surg Br 85(2):223–230
Noyes FR, McGinniss GH, Mooar LA (1984) Functional disability in the anterior cruciate insufficient knee syndrome: review of knee rating systems and projected risk factors in determining treatment. Sports Med 1(4):278–302
Agel J, LaPrade RF (2009) Assessment of differences between the modified Cincinnati and International Knee Documentation Committee patient outcome scores: a prospective study. Am J Sport Med 37(11):2151–2157
Saragaglia D (2012) Les ruptures récentes et anciennes de l’appareil extenseur du genou de l’adulte (hors prothèses). In: Conférence Enseign
Vidil A, Ouaknine M, Anract P (2004) Ruptures traumatiques du tendon quadricipital: a propos de 47 cas. Rev Chir Orthop 90:40–48
Rougraff BT, Reeck CC, Essenmacher J (1996) Complete quadriceps tendon ruptures. Orthopedics 19(6):509–514
Vainionpää S (1985) Rupture of the quadriceps tendon. Acta Orthop Scand 56:433–435
Siwek CW, Rao JP (1981) Ruptures of the extensor mechanism of the knee joint. J Bone Jt Surg Am 63:932–937
Ilan DI, Tejwani N, Keschner M (2003) Quadriceps tendon rupture. J Am Acad Orthop Surg 11(3):192–200
He L, Wang T, Wang M, Rong G (2002) Patella ligament and femoral quadriceps tendon rupture. Zhonghua Wai Ke Za Zhi 40(12):918–922
Lee D, Stinner D, Mir H (2013) Quadriceps and patellar tendon ruptures. J Knee Surg 26(5):301–308
Wenzl ME, Kirchner R, Seide K (2004) Quadriceps tendon ruptures—is there a complete functional restitution? Injury 35:922–926
Sommelet J, Fery G, Grosdidier G (1979) Des ruptures de l’appareil extenseur du genou: a propos de 45 cas. Int Orthop 3:27–36
Duthon VB, Fritschy D (2011) Ruptures de l’appareil extenseur du genou. Rev Méd Suisse 7:1544–1548
Lerais JM, Krause D, Kastler B, Tavernier C (2009) Pathologie péri-articulaire du genou. Pathologie articulaire et péri articulaire des membres Clinique, imagerie diagnostique et thérapeutique. Masson, pp 425–429
Ciriello V, Gudipati S, Tosounidis T (2012) Clinical outcomes after repair of quadriceps tendon rupture: a systematic review. Injury 43:1931–1938
Maffulli N, Del Buono A, Spieza F (2012) Light microscopic histology of quadriceps tendon ruptures. Int Orthop 36:2367–2371
Delafenêtre MI, Massy N, Thuillez C, Noblet C (2008) Tendinous disorders attributed to statins: a study on ninety-six spontaneous reports in the period 1990–2005 and review of the literature. Arthritis Rheum 59(3):367–372
Ho HM, Lee WKE (2003) Traumatic bilateral concurrent patellar tendon rupture: an alternative fixation method. Knee Surg Sports Traumatol Arthrosc 11:105–111
Capiola D, Re L (2007) Repair of patellar tendon rupture with suture anchors. Arthroscopy 23(8):906.e1–906.e4
Boudissa M, Roudet A, Rubens-Duval B (2014) Ruptures aiguës du tendon quadrcipital: une série de 50 genoux à plus de 6 ans. Rev Chir Orthop 100:171–174
Barber FA, Herbert MA, Click JN (1997) Internal fixation strength of suture anchors—update 1997. Arthroscopy 13(3):355–362
Barber FA, Herbert MA, Coons DA (2006) Sutures and suture anchors—update 2006. Arthroscopy 22(10):1063.e1–9
Bisbinas I, Magnissalis E, Gigis I (2013) Rotator cuff repair: a biomechanical ex vivo ovine study. Proc Inst Mech Eng H 227(5):560–570
Tingart MJ, Apreleva M, Lehtinen J (2004) Anchor design an bone mineral density affect the pull-out strength of suture anchors in rotator cuff repair: which anchors are best to use in patients with low bone quality? Am J Sport Med 32(6):1466–1473
Barber FA, Herbert MA, Hapa O (2011) Biomechanical analysis of pullout strengths of rotator cuff and glenoid anchors: 2011 update. Arthroscopy 27(7):895–905
Rehby L, Lepage D, Sarlieve P (2007) Imagerie du tendon du biceps brachial réinséré par ancre: la fixation est-elle viable? Bioingénierie et reconstruction osseuse. Sauramps Medical, pp 167–174
Gallinet D, Dietsch E, Barbier-Brion B (2011) Suture anchor reinsertion of distal biceps rupture: clinical results and radiological assessment of tendon healing. Orthop Traumatol Surg Res 97:252–259
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethical statement
Ethical standards declaration EJOST fully adopts and supports ethical standards of the responsible committee on human experimentation (institutional and national with respect to each author) and the Helsinki Declaration of 1975, as revised in 2000. Authors indicate that all their experiments on human subjects published in this article are in accordance with these standards. In case of any doubt, the authors agree to explain the rationale for their approach and demonstrate that the institutional review body explicitly approved the doubtful aspects of the study. When reporting experiments on animals, authors will indicate whether the institutional and national guide for the care and use of laboratory animals was followed. Further, EJOST fully adopts and supports the standards of the International Committee of Medical Journal Editors. Authors agree to handle the statement of informed consent as indicated in the instructions to authors with regard to privacy and confidentiality of patients mentioned in the text. When informed consent has been obtained, it will be indicated in the published article.
Statement of informed consent
Patients have a right to privacy that should not be infringed without informed consent. Identifying information, including patients’ names, initials or hospital numbers, should not be published in written descriptions, photographs and pedigrees unless the information is essential for scientific purposes and the patient (or parent or guardian) gives written informed consent for publication. Informed consent for this purpose requires that a patient who is identifiable be shown the manuscript to be published. Authors should identify individuals who provide writing assistance and disclose the funding source for this assistance. Identifying details should be omitted if they are not essential. Complete anonymity is difficult to achieve, however, and informed consent should be obtained if there is any doubt. For example, masking the eye region in photographs of patients is inadequate protection of anonymity. If identifying characteristics are altered to protect anonymity, such as in genetic pedigrees, authors should provide assurance that alterations do not distort scientific meaning and editors should so note.
Rights and permissions
About this article

Cite this article
Mille, F., Adam, A., Aubry, S. et al. Prospective multicentre study of the clinical and functional outcomes following quadriceps tendon repair with suture anchors. Eur J Orthop Surg Traumatol 26, 85–92 (2016). https://doi.org/10.1007/s00590-015-1710-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-015-1710-6