
Abstract
Purpose
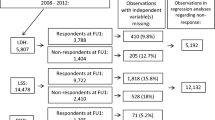
Lumbar spinal stenosis (LSS) can be surgically treated, with variable outcome. Studies have linked socioeconomic factors to outcome, but no nation-wide studies have been performed. This register-based study, including all patients surgically treated for LSS during 2008–2012 in Sweden, aimed to determine predictive factors for the outcome of surgery.
Methods
Clinical and socioeconomic factors with impact on outcome in LSS surgery were identified in several high-coverage registers, e.g., the national quality registry for spine surgery (Swespine, FU-rate 70–90%). Multivariate regression analyses were conducted to assess their effect on outcome. Two patient-reported outcome measures, Global Assessment of leg pain (GA) and the Oswestry Disability Index (ODI), as well as length of sick leave after surgery were analyzed.
Results
Clinical and socioeconomic factors significantly affected health outcome (both GA and ODI). Some predictors of a good outcome (ODI) were: being born in the EU, reporting no back pain at baseline, a high disposable income and a high educational level. Some factors predicting a worse outcome were previous surgery, having had back pain more than 2 years, having comorbidities, being a smoker, being on social welfare and being unemployed.
Conclusions
The study highlights the relevance of adding socioeconomic factors to clinical factors for analysis of patient-reported outcomes, although the causal pathway of most predictors’ impact is unknown. These findings should be further investigated in the perspective of treatment selection for individual LSS patients. The study also presents a foundation of case mix algorithms for predicting outcome of surgery for LSS.
Graphical abstract
These slides can be retrieved under Electronic Supplementary Material.




Similar content being viewed by others


Notes
Question: How is your leg/back pain today compared to before surgery? Possible answers: 0 = no pain before surgery (not included in statistical model), 1 = pain free, 2 = much improved, 3 = somewhat improved, 4 = unchanged, 5 = worse.
High score = high disability.
The first 14 days of sick-leave is not reported to the Swedish Social Insurance Agency, hence not accounted for in these analyses.
Retirement age in Sweden.
Elixhauser index, method for measuring patient comorbidity based on diagnosis codes in administrative data (includes mental disorders, drug and alcohol abuse, obesity, coagulopathy, weight loss and fluid and electrolyte disorders).
References
Amundsen T, Weber H, Lilleas F, Nordal HJ, Abdelnoor M, Magnaes B (1995) Lumbar spinal stenosis. Clinical and radiologic features. Spine (Phila Pa 1976) 20(10):1178–1186
Stromqvist B, Fritzell P, Hagg O, Jonsson B, Sanden B, Swedish Society of Spinal S (2013) Swespine: the Swedish spine register: the 2012 report. Eur Spine J 22(4):953–974
Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Blood E, Hanscom B et al (2008) Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med 358(8):794–810
Försth P, Olafsson G, Carlsson T, Frost A, Borgström F, Fritzell P et al (2016) A randomized controled trial of fusion surgery for lumbar spinal stenosis. N Engl J Med 374(15):1413–1423
Iversen MD, Daltroy LH, Fossel AH, Katz JN (1998) The prognostic importance of patient pre-operative expectations of surgery for lumbar spinal stenosis. Patient Educ Couns 34(2):169–178
Abbott AD, Tyni-Lenne R, Hedlund R (2010) The influence of psychological factors on pre-operative levels of pain intensity, disability and health-related quality of life in lumbar spinal fusion surgery patients. Physiotherapy 96(3):213–221
Knutsson B, Michaelsson K, Sanden B (2013) Obesity is associated with inferior results after surgery for lumbar spinal stenosis: a study of 2633 patients from the Swedish spine register. Spine (Phila Pa 1976) 38(5):435–441
Sanden B, Forsth P, Michaelsson K (2011) Smokers show less improvement than nonsmokers two years after surgery for lumbar spinal stenosis: a study of 4555 patients from the Swedish spine register. Spine (Phila Pa 1976) 36(13):1059–1064
Stromqvist F, Ahmad M, Hildingsson C, Jonsson B, Stromqvist B (2008) Gender differences in lumbar disc herniation surgery. Acta Orthop 79(5):643–649
Cobo Soriano J, Sendino Revuelta M, Fabregate Fuente M, Cimarra Diaz I, Martinez Urena P, Deglane Meneses R (2010) Predictors of outcome after decompressive lumbar surgery and instrumented posterolateral fusion. Eur Spine J 19(11):1841–1848
Fritzell P, Hagg O, Wessberg P, Nordwall A, Swedish Lumbar Spine Study G (2001) Volvo Award Winner in Clinical Studies: lumbar fusion versus nonsurgical treatment for chronic low back pain: a multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine (Phila Pa 1976) 26(23):2521–2532 (discussion 32-4)
Fairbank JC, Couper J, Davies JB, O’Brien JP (1980) The Oswestry low back pain disability questionnaire. Physiotherapy 66(8):271–273
EuroQol G (1990) EuroQol—a new facility for the measurement of health-related quality of life. Health Policy 16(3):199–208
Huskisson EC (1974) Measurement of pain. Lancet 2(7889):1127–1131
Elixhauser A, Steiner C, Harris DR, Coffey RM (1998) Comorbidity measures for use with administrative data. Med Care 36(1):8–27
Hermansen E, Romild UK, Austevoll IM, Solberg T, Storheim K, Brox JI et al (2017) Does surgical technique influence clinical outcome after lumbar spinal stenosis decompression? A comparative effectiveness study from the Norwegian Registry for Spine Surgery. Eur Spine J 26(2):420–427
Mobbs RJ, Li J, Sivabalan P, Raley D, Rao PJ (2014) Outcomes after decompressive laminectomy for lumbar spinal stenosis: comparison between minimally invasive unilateral laminectomy for bilateral decompression and open laminectomy: clinical article. J Neurosurg Spine. 21(2):179–186
Hagg O, Fritzell P, Oden A, Nordwall A, Swedish Lumbar Spine Study G (2002) Simplifying outcome measurement: evaluation of instruments for measuring outcome after fusion surgery for chronic low back pain. Spine (Phila Pa 1976) 27(11):1213–1222
Hedlund R, Johansson C, Hagg O, Fritzell P, Tullberg T, Swedish Lumbar Spine Study G (2016) The long-term outcome of lumbar fusion in the Swedish lumbar spine study. Spine J 16(5):579–587
Gunzburg R, Szpalski M (2003) The conservative surgical treatment of lumbar spinal stenosis in the elderly. Eur Spine J 12(Suppl 2):S176–S180
King MT (2011) A point of minimal important difference (MID): a critique of terminology and methods. Expert Rev Pharmacoecon Outcomes Res 11(2):171–184
Parker SL, Adogwa O, Mendenhall SK, Shau DN, Anderson WN, Cheng JS et al (2012) Determination of minimum clinically important difference (MCID) in pain, disability, and quality of life after revision fusion for symptomatic pseudoarthrosis. Spine J 12(12):1122–1128
Ghogawala Z, Benzel EC, Amin-Hanjani S, Barker FG 2nd, Harrington JF, Magge SN et al (2004) Prospective outcomes evaluation after decompression with or without instrumented fusion for lumbar stenosis and degenerative Grade I spondylolisthesis. J Neurosurg Spine 1(3):267–272
Herkowitz HN, Kurz LT (1991) Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 73(6):802–808
Forsth P, Michaelsson K, Sanden B (2013) Does fusion improve the outcome after decompressive surgery for lumbar spinal stenosis?: a two-year follow-up study involving 5390 patients. Bone Joint J 95-B(7):960–965
Piha K, Laaksonen M, Martikainen P, Rahkonen O, Lahelma E (2010) Interrelationships between education, occupational class, income and sickness absence. Eur J Public Health 20(3):276–280
Solberg TK, Sorlie A, Sjaavik K, Nygaard OP, Ingebrigtsen T (2011) Would loss to follow-up bias the outcome evaluation of patients operated for degenerative disorders of the lumbar spine? Acta Orthop 82(1):56–63
Acknowledgements
The authors thank Swespine, Swedish Society of Spinal Surgery (4 s) and all participating county councils. Partial funding from Forte programme Grant 2012/1688 (“Value and choice”) is gratefully acknowledged.
Funding
Funding for this research was provided by Sveus, through the Ministry of Health and Social Affairs (Dnr S2012/8356/FS) and seven Swedish regions. Sveus is a research collaboration in which seven Swedish regions develop systems for value-based monitoring of health care. The overarching aim of Sveus is to stimulate a value-driven, efficient and patient-centered health care, and the work has been carried out for a number of different patient groups, of which spine surgery is one.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
HI, CW and FB are employees at Ivbar Institute (a healthcare research consultancy), which has received research grants from Sveus (county council consortium) for the submitted work. FB holds shares in Ivbar Institute. The other authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Iderberg, H., Willers, C., Borgström, F. et al. Predicting clinical outcome and length of sick leave after surgery for lumbar spinal stenosis in Sweden: a multi-register evaluation. Eur Spine J 28, 1423–1432 (2019). https://doi.org/10.1007/s00586-018-5842-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-018-5842-3