
Abstract
Purpose
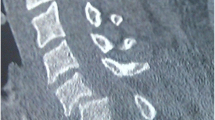
Surgical reduction of uni and bi-facetal dislocations of the cervical spine (AO type C injuries) can be performed by posterior, anterior or combined approaches. Ease of access, low infection rates and less risks of neurological worsening has popularized anterior approach. However, the reduction of locked cervical facets can be intricate through anterior approach. We analyzed the safety, efficacy and outcomes at a minimum 1 year, of a novel anterior reduction technique for consecutively treated cervical facet dislocations.
Materials and methods
Patients with single level traumatic sub-axial cervical dislocation (n = 39) treated by this modified anterior technique were studied. The technique involved standard Smith–Robinson approach, discectomy beyond PLL, use of inter-laminar distracter to distract while Caspar pins were used as “joysticks” (either flexion–extension or lateral rotation moments are provided), to reduce the sub-luxed facets. Among 51 patients with cervical type C injury treated during the study period, 4 patients who had spontaneous reduction and 8 treated by planned global fusion were excluded.
Results
39 patients of mean age 49.9 years were studied. The levels of injury included (C3–4 = 2, C4–5 = 5, C5–6 = 20, C6–7 = 12). 18 were bi-facetal and 21 were uni-facetal dislocation. One facet was fractured in 17 and both in 5 patients. 30% (n = 13) had a concomitant disc prolapse. The neurological status was as follows: 9 ASIA A, 9 ASIA C, 13 ASIA D and 8 ASIA E. All the patients were successfully reduced by this technique and fixed with anterior locking cervical locking plates. No supplemental posterior surgery was performed. 22 patients with incomplete deficit showed recovery. The mean follow-up was 14.3 months and there was no implant failure except one patient who had partial loss of the reduction.
Conclusion
Patients with traumatic sub-axial cervical dislocation (AO type C injuries) can be safely and effectively reduced by this technique. Other advantages include minimal blood loss, less risks of infection, shorted fusion zone, good fusion rate and neurological recovery.





Similar content being viewed by others


References
Beyer CA, Cabanela ME, Berquist TH (1991) Unilateral facet dislocations and fracture-dislocations of the cervical spine. J Bone Joint Surg Br 73:977–981
Cotler JM, Herbison GJ, Nasuti JF et al (1993) Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 18:386–390
Caspar W, Barbier DD, Klara PM (1989) Anterior cervical fusion and Caspar plate stabilization for cervical trauma. Neurosurgery 25:491–502
Hadley MN, Fitzpatrick BC, Sonntag VK, Browner CM (1992) Facet fracture-dislocation injuries of the cervical spine. Neurosurgery 30:661–666
Eismont FJ, Arena MJ, Green BA (1991) Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. Case report. J Bone Joint Surg Am 73:1555–1560
Kleyn PJ (1984) Dislocations of the cervical spine: closed reduction under anaesthesia. Paraplegia 22:271–281. https://doi.org/10.1038/sc.1984.45
de Oliveira JC (1979) Anterior reduction of interlocking facets in the lower cervical spine. Spine 4:195–202
Robertson PA, Ryan MD (1992) Neurological deterioration after reduction of cervical subluxation. Mechanical compression by disc tissue. J Bone Joint Surg Br 74:224–227
Olerud C, Jónsson H (1991) Compression of the cervical spine cord after reduction of fracture dislocations. Report of 2 cases. Acta Orthop Scand 62:599–601
Rizzolo SJ, Piazza MR, Cotler JM et al (1991) Intervertebral disc injury complicating cervical spine trauma. Spine 16:S187–S189
Olsen MA, Mayfield J, Lauryssen C et al (2003) Risk factors for surgical site infection in spinal surgery. J Neurosurg 98:149–155
Wimmer C, Gluch H, Franzreb M, Ogon M (1998) Predisposing factors for infection in spine surgery: a survey of 850 spinal procedures. J Spinal Disord 11:124–128
Pull ter Gunne AF, Cohen DB (2009) Incidence, prevalence, and analysis of risk factors for surgical site infection following adult spinal surgery. Spine 34:1422–1428. https://doi.org/10.1097/BRS.0b013e3181a03013
Fountas KN, Kapsalaki EZ, Nikolakakos LG et al (2007) Anterior cervical discectomy and fusion associated complications. Spine 32:2310–2317. https://doi.org/10.1097/BRS.0b013e318154c57e
Barnes M, Liew S (2012) The incidence of infection after posterior cervical spine surgery: a 10 year review. Glob Spine J 2:3–6. https://doi.org/10.1055/s-0032-1307252
Ordonez BJ, Benzel EC, Naderi S, Weller SJ (2000) Cervical facet dislocation: techniques for ventral reduction and stabilization. J Neurosurg 92:18–23
Funding
The study was funded by the Ganga Orthopaedic Research and Education Foundation (GOREF).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Kanna, R.M., Shetty, A.P. & Rajasekaran, S. Modified anterior-only reduction and fixation for traumatic cervical facet dislocation (AO type C injuries). Eur Spine J 27, 1447–1453 (2018). https://doi.org/10.1007/s00586-017-5430-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-017-5430-y