
Abstract
Background
Adult spinal deformity (ASD) is a major public health problem. There are pros and cons of the available treatment alternatives (surgical or non-surgical) and it had been difficult to identify the best treatment modality.
Aim
To construct a statistical DA model to identify the optimum overall treatment in ASD.
Methods
From an international multicentre database of ASD patients (968 pts), 535 who had completed 1 year follow-up (371 non-surgical—NS, 164 surgical—S), constitute the population of this study. DA was structured in two main steps of: (1) baseline analysis (assessing the probabilities of outcomes, assessing the values of preference—utilities-, combining information on probability and utility and assigning the quality adjusted life expectancy (QALE) for each treatment) and (2) sensitivity analysis.
Results
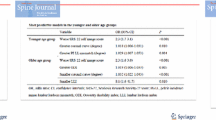
Four hundred and thirty-two patients (309 NS, 123 S) had baseline and 1 year follow-up ODI measurements. Overall, 104 (24.1 %) were found to be improved (a decrease in ODI > 8 points), 225 (52.1 %) unchanged (−8 > ODI > 8) and 65 deteriorated. Surgery presented with a higher chance of improvement (54.2 %) versus NS (9.7 %). The overall QALE ranged from 56 to 69 (of 100 years) and demonstrated better final QALE in the NS group (60 vs. 65, P = 0.0038), this group having started with higher QALE as well (56 vs. 65 years, P < 0.0001). There were improvements in overall QALE in both groups but this was significant only in the surgical group (S from 56 to 60 years, P < 0.0001; NS from 65 to 65 years, P = 0.27). In addition, in the subgroup of patients with significant baseline disability (ODI > 25) surgery appeared to yield marginally better final QALE (58 vs. 56 years, P = 0.1) despite very a similar baseline (54 vs. 54 years, P = 0.93).
Discussion and conclusions
This study demonstrated that a single best treatment modality for ASD may not exist. Conservative treatment appears to yield higher (up to 6 %) QALE compared to surgery, most probably secondary to a higher baseline QALE. On the other hand, surgery provides a significantly higher increase in QALE. Especially in patients with significant disability at baseline, the final QALE tended higher in the S group (although not significant). Finally, chances of a relevant improvement at first year turned out to be significantly lower with NS treatment.


Similar content being viewed by others


References
Acaroglu E, Guler UO, Olgun DZ, Yavuz Y, Pellise F, Domingo-Sabat M, Yakiici S, Alanay A, Perez-Grueso FS, Yavuz Y, European Spine Study Group (2015) Multiple regression analysis of factors affecting HRQL in adult spinal deformity (ASD). Spine Deformity 3:360–366
Pellise F, Vila-Casademunt A, Ferrer M, Domingo-Sàbat M, Bagó J, Pérez-Grueso FJ, Alanay A, Mannion AF, Acaroglu E, European Spine Study Group (ESSG) (2014) Impact on health related quality of life of adult spinal deformity (ASD) compared with other chronic conditions. Eur Spine J. 24(1), pp. 3–11, doi:10.1007/s00586-014-3542-1
Good CR, Auerbach JD, O’Leary PT, Schuler TC (2011) Adult spine deformity. Curr Rev Musculoskelet Med 4:159–167
Everett CR, Patel RK (2007) A systematic literature review of nonsurgical treatment in adult scoliosis. Spine 32(19 Suppl):S130–S134
Bridwell KH, Glassman S, Horton W, Shaffrey C, Schwab F, Zebala LP, Lenke LG, Hilton JF, Shainline M, Baldus C, Wootten D (2009) Does treatment (nonoperative and operative) improve the two-year quality of life in patients with adult symptomatic lumbar scoliosis: a prospective multicenter evidence-based medicine study. Spine 34(20):2171–2178
Daubs MD, Lenke LG, Cheh G, Stobbs G, Bridwell KH (2007) Adult spinal deformity surgery: complications and outcomes in patients over age 60. Spine 32(20):2238–2244
Parker SL, Mendenhall SK, Shau D, Adogwa O, Cheng JS, Anderson WN, Devin CJ, McGirt MJ (2012) Determination of minimum clinically important difference in pain, disability, and quality of life after extension of fusion for adjacent-segment disease. J Neurosurg Spine 1:61–67. doi:10.3171/2011.8.SPINE1194
Patel MS, Newey M, Sell P (2013) Minimum clinically important differences in spinal surgery. Bone Joint J 95-B(Suppl 4):15
Acaroglu E, Guler UO, Cetinyurek-Yavuz A, Yuksel S, Yavuz Y, Domingo-Sabat M, Pellise F, Alanay A, Perez-Grueso F, Kleinstück F, Obeid I, ESSG (2015) Decision analysis to identify the ideal treatment for adult spinal deformity: what is the impact of complications on patient outcomes? (Unpublished data, in review in Global Spine Journal)
DiCenso A, Cullum N, Ciliska D (1998) Implementing evidence based nursing: some misconceptions. Evid Based Nurs 1:38–39
Brazier JE, Green C, Kanis JA, Committee of Scientific Advisors International Osteoporosis Foundation (2002) A systematic review of health state utility values for osteoporosis-related conditions. Osteoporos Int 13(10):768–776
Brazier J, Roberts J, Deverill M (2002) The estimation of a preference-based measure of health from the SF-36. J Health Econ 2:271–292
Acknowledgments
This study was funded by a research grant from the Spine Society of Europe (2013). European Spine Study Group is funded by a research grant from Johnson and Johnson Depuy-Synthes.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Acaroglu, E., Yavuz, A.C., Guler, U.O. et al. A decision analysis to identify the ideal treatment for adult spinal deformity: is surgery better than non-surgical treatment in improving health-related quality of life and decreasing the disease burden?. Eur Spine J 25, 2390–2400 (2016). https://doi.org/10.1007/s00586-016-4413-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-016-4413-8